

Impacts of embracing 39-week elective induction across an entire labor and delivery unit
- PMID: 36941864
- PMCID: PMC10024218
- DOI: 10.1016/j.xagr.2023.100168
Impacts of embracing 39-week elective induction across an entire labor and delivery unit
Abstract
Background: Induction of labor among low-risk, 39-week nulliparas increased significantly in the United States following publication of the outcomes of A Randomized Trial of Induction Versus Expectant Management trial. However, the rates of labor induction and outcomes in non-nulliparous patients and the wider impacts on the labor unit have not been reported widely.
Objective: This study aimed to compare the induction of labor rates and outcomes before and after liberal implementation of 39-week elective induction at a single center.
Study design: This was a retrospective cohort study comparing the delivery characteristics of pregnancies 1 year before and 1 year after adoption of a new 39-week elective induction policy at a single, tertiary-care center. Notably, elective induction was not restricted to nulliparas. We examined all live, singleton, in-born deliveries ≥36 weeks gestation, excluding those with fetal anomalies and prolonged antenatal admission. Deliveries at ≥39 weeks gestation were further subcategorized as being high risk (diabetes mellitus, chronic hypertension, intrauterine growth restriction, history of fetal demise or cholestasis) or low risk, nulliparas vs multiparas, and with or without a previous cesarean delivery. Elective deliveries were those without a maternal, fetal, or obstetrical indication. Primary outcomes included gestational age and indications for delivery, rates of labor induction and elective induction, and time from admission to delivery. Secondary outcomes included the rate of cesarean deliveries, indications for cesarean deliveries, and maternal and newborn morbidities. The outcomes were compared using Wilcoxon rank-sum tests or chi-square tests as appropriate. The odds of cesarean delivery were analyzed using multivariate logistic regression and controlling for relevant confounders.
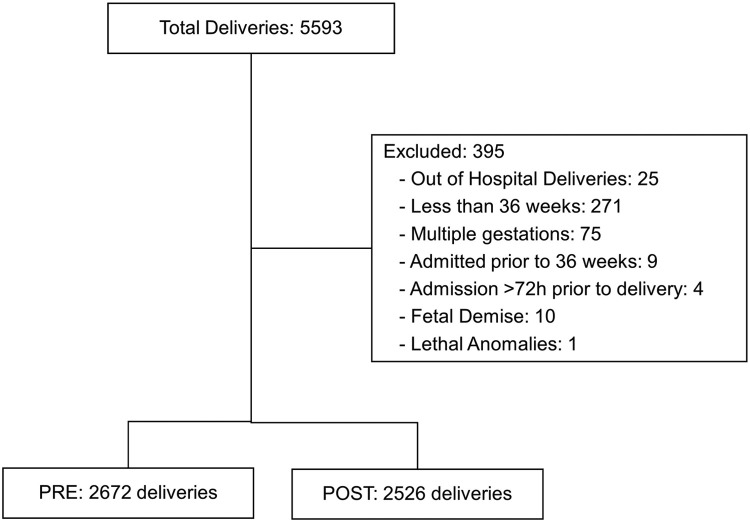
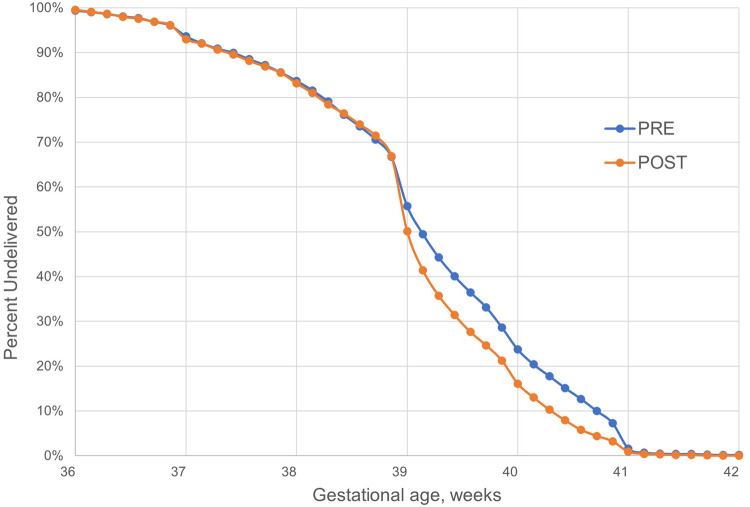
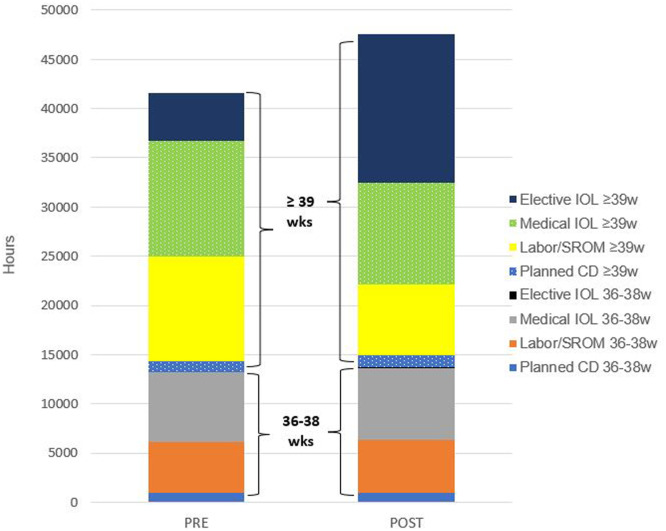
Results: A total of 2672 pre-implementation and 2526 post-implementation deliveries were studied. Among patients at ≥39 weeks gestation, elective delivery increased (pre-implementation, 344/1788 [19.2%] vs post-implementation, 684/1710 [40.0%]; P<.01) and admission for labor or ruptured membranes decreased (pre-implementation, 920/1788 [51.5%] vs post-implementation, 579/1710 [33.9%]; P<.01). Labor induction in the 39th week of gestation increased among low-risk and high-risk nulliparas, multiparas, and those with a previous cesarean delivery (P<.05 for each pairwise comparison), and the rate of 39-week elective inductions increased in all low-risk subgroups. Deliveries at 36 to 38 weeks gestation were similar in the proportion, timing, indications for delivery, and rate of labor induction. The odds of cesarean delivery was unchanged overall (adjusted odds ratio, 0.97; 95% confidence interval, 0.83-1.14) and for low-risk, ≥39-week nulliparas (adjusted odds ratio, 0.90; 95% confidence interval, 0.66-1.23) and low-risk, ≥39-week multiparas (adjusted odds ratio, 1.18; 95% confidence interval, 0.71-1.98). Among all deliveries, the median (interquartile range) time from admission to delivery increased significantly (pre-implementation, 12.8 [6.0-21.6] hours vs post-implementation, 15.6 [7.1-25.1] hours; P<.01) and the total cumulative patient care time from admission to delivery increased by 15% (pre-implementation, 41,578 hours vs post-implementation, 47,605 hours) when normalized by delivery volume. Chorioamnionitis incidence increased, whereas other maternal and neonatal morbidities were unchanged.
Conclusion: Following adoption of a nonrestrictive, 39-week elective induction policy at a single, tertiary-care center, the rates of 39-week induction of labor and elective inductions increased among nulliparas, multiparas, and those with a previous cesarean delivery. The rate of cesarean delivery was unchanged, and the median time from admission to delivery and the cumulative admission to delivery hours increased significantly. Future studies are needed to further explore the full scope of the impacts on labor unit operations, costs, and patient experiences and outcomes.
Keywords: 39 weeks; A Randomized Trial of Induction Versus Expectant Management trial; cesarean; low risk; nullipara.
© 2023 The Authors.
Figures
Comment in
-
Excerpts from the World Medical Literature: Obstetrics.J Obstet Gynaecol Can. 2023 Jul;45(7):479-481. doi: 10.1016/j.jogc.2023.04.018. J Obstet Gynaecol Can. 2023. PMID: 37400184 No abstract available.
References
-
- Gilroy LC, Al-Kouatly HB, Minkoff HL, Mclaren RA. Changes in obstetrical practices and pregnancy outcomes following the ARRIVE trial. Am J Obstet Gynecol. 2022;226:716. e1–12. - PubMed
-
- Medically indicated late-preterm and early-term deliveries: ACOG committee Opinion, Number 818. Obstet Gynecol. 2021;137:e29–e33. - PubMed
-
- Sophia Y, Rishi B, James B, Andrea J. Universal testing for severe acute respiratory syndrome coronavirus 2 upon admission to three labor and delivery units in Santa Clara County, CA. Clin J Obstet Gynecol. 2020;3:109–113.
-
- Rossi RM, Requarth E, Warshak CR, Dufendach KR, Hall ES, DeFranco EA. Risk calculator to predict cesarean delivery among women undergoing induction of labor. Obstet Gynecol. 2020;135:559–568. - PubMed
LinkOut - more resources
Full Text Sources
