

The architecture of abnormal reward behaviour in dementia: multimodal hedonic phenotypes and brain substrate
- PMID: 36942157
- PMCID: PMC10023829
- DOI: 10.1093/braincomms/fcad027
The architecture of abnormal reward behaviour in dementia: multimodal hedonic phenotypes and brain substrate
Abstract
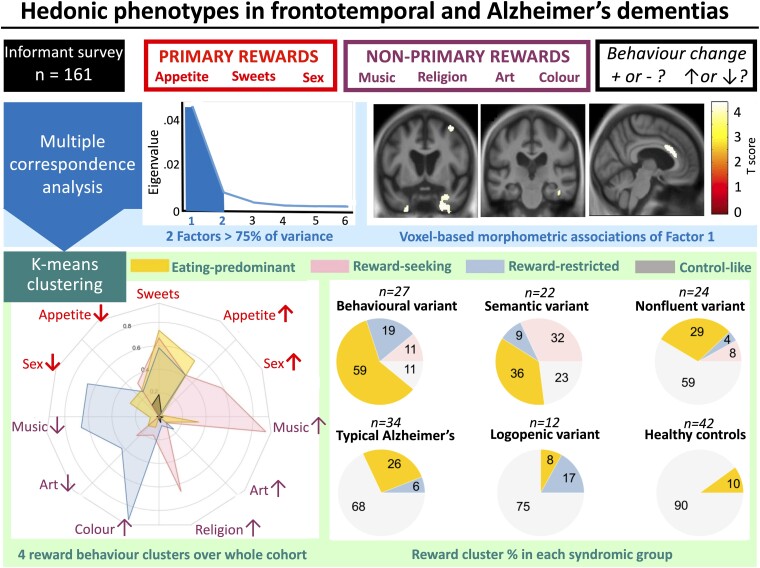
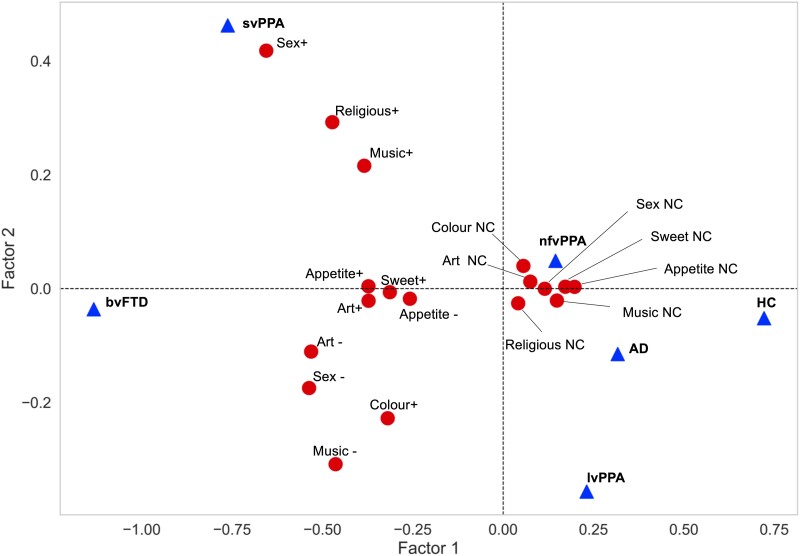
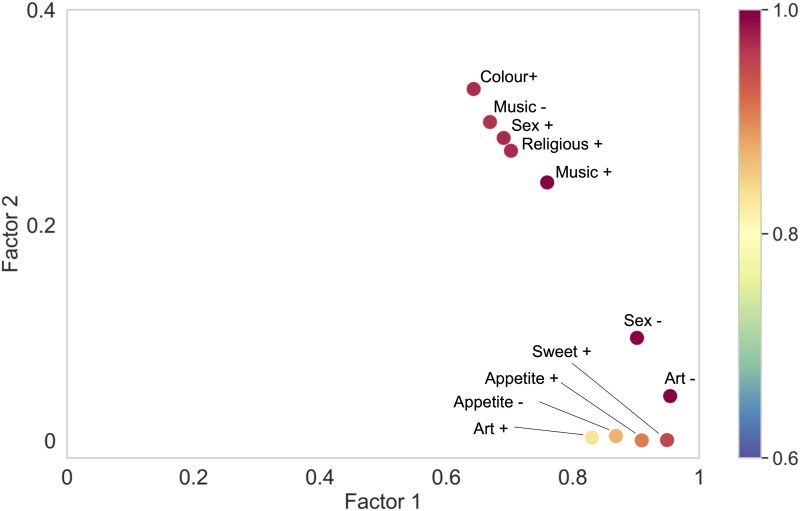
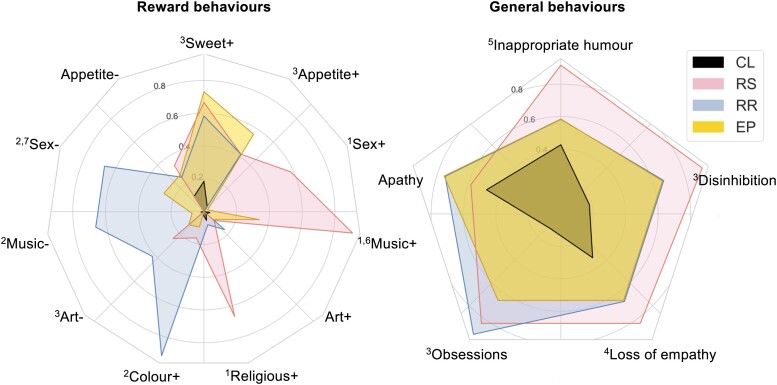
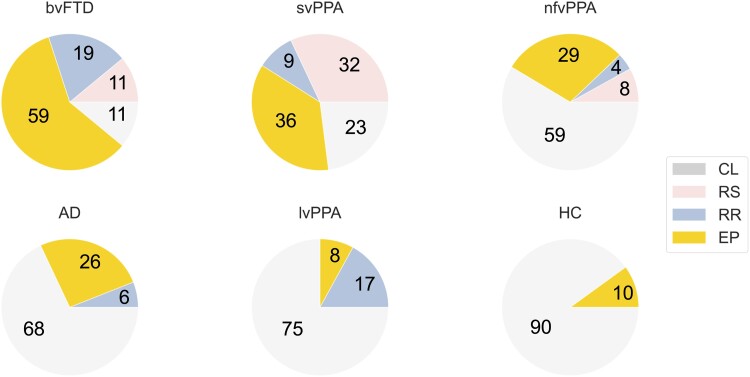
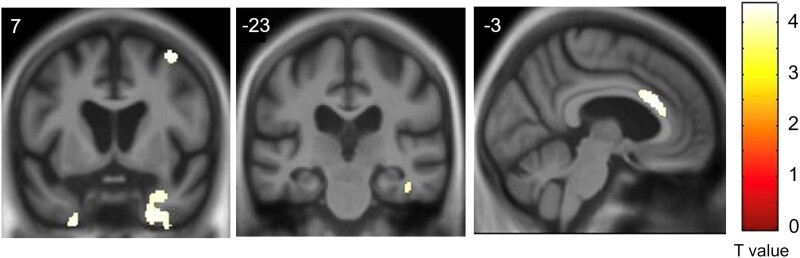
Abnormal reward processing is a hallmark of neurodegenerative diseases, most strikingly in frontotemporal dementia. However, the phenotypic repertoire and neuroanatomical substrates of abnormal reward behaviour in these diseases remain incompletely characterized and poorly understood. Here we addressed these issues in a large, intensively phenotyped patient cohort representing all major syndromes of sporadic frontotemporal dementia and Alzheimer's disease. We studied 27 patients with behavioural variant frontotemporal dementia, 58 with primary progressive aphasia (22 semantic variant, 24 non-fluent/agrammatic variant and 12 logopenic) and 34 with typical amnestic Alzheimer's disease, in relation to 42 healthy older individuals. Changes in behavioural responsiveness were assessed for canonical primary rewards (appetite, sweet tooth, sexual activity) and non-primary rewards (music, religion, art, colours), using a semi-structured survey completed by patients' primary caregivers. Changes in more general socio-emotional behaviours were also recorded. We applied multiple correspondence analysis and k-means clustering to map relationships between hedonic domains and extract core factors defining aberrant hedonic phenotypes. Neuroanatomical associations were assessed using voxel-based morphometry of brain MRI images across the combined patient cohort. Altered (increased and/or decreased) reward responsiveness was exhibited by most patients in the behavioural and semantic variants of frontotemporal dementia and around two-thirds of patients in other dementia groups, significantly (P < 0.05) more frequently than in healthy controls. While food-directed changes were most prevalent across the patient cohort, behavioural changes directed toward non-primary rewards occurred significantly more frequently (P < 0.05) in the behavioural and semantic variants of frontotemporal dementia than in other patient groups. Hedonic behavioural changes across the patient cohort were underpinned by two principal factors: a 'gating' factor determining the emergence of altered reward behaviour and a 'modulatory' factor determining how that behaviour is directed. These factors were expressed jointly in a set of four core, trans-diagnostic and multimodal hedonic phenotypes: 'reward-seeking', 'reward-restricted', 'eating-predominant' and 'control-like'-variably represented across the cohort and associated with more pervasive socio-emotional behavioural abnormalities. The principal gating factor was associated (P < 0.05 after correction for multiple voxel-wise comparisons over the whole brain) with a common profile of grey matter atrophy in anterior cingulate, bilateral temporal poles, right middle frontal and fusiform gyri: the cortical circuitry that mediates behavioural salience and semantic and affective appraisal of sensory stimuli. Our findings define a multi-domain phenotypic architecture for aberrant reward behaviours in major dementias, with novel implications for the neurobiological understanding and clinical management of these diseases.
Keywords: Alzheimer’s disease; frontotemporal dementia; primary progressive aphasia; reward; semantic dementia.
© The Author(s) 2023. Published by Oxford University Press on behalf of the Guarantors of Brain.
Conflict of interest statement
The authors report no conflict of interest.
Figures
Comment on
-
Reconciling profiles of reward-seeking versus reward-restricted behaviours in frontotemporal dementia.Brain Commun. 2023 Mar 1;5(2):fcad045. doi: 10.1093/braincomms/fcad045. eCollection 2023. Brain Commun. 2023. PMID: 36938524 Free PMC article.
References
-
- Sivasathiaseelan H, Marshall CR, Agustus JL, et al. . Frontotemporal dementia: A clinical review. Semin Neurol. 2019;39(2):251–263. - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources