

Efficacy and Safety of Early Administration of 4-Factor Prothrombin Complex Concentrate in Patients With Trauma at Risk of Massive Transfusion: The PROCOAG Randomized Clinical Trial
- PMID: 36942533
- PMCID: PMC10031505
- DOI: 10.1001/jama.2023.4080
Efficacy and Safety of Early Administration of 4-Factor Prothrombin Complex Concentrate in Patients With Trauma at Risk of Massive Transfusion: The PROCOAG Randomized Clinical Trial
Abstract
Importance: Optimal transfusion strategies in traumatic hemorrhage are unknown. Reports suggest a beneficial effect of 4-factor prothrombin complex concentrate (4F-PCC) on blood product consumption.
Objective: To investigate the efficacy and safety of 4F-PCC administration in patients at risk of massive transfusion.
Design, setting, and participants: Double-blind, randomized, placebo-controlled superiority trial in 12 French designated level I trauma centers from December 29, 2017, to August 31, 2021, involving consecutive patients with trauma at risk of massive transfusion. Follow-up was completed on August 31, 2021.
Interventions: Intravenous administration of 1 mL/kg of 4F-PCC (25 IU of factor IX/kg) vs 1 mL/kg of saline solution (placebo). Patients, investigators, and data analysts were blinded to treatment assignment. All patients received early ratio-based transfusion (packed red blood cells:fresh frozen plasma ratio of 1:1 to 2:1) and were treated according to European traumatic hemorrhage guidelines.
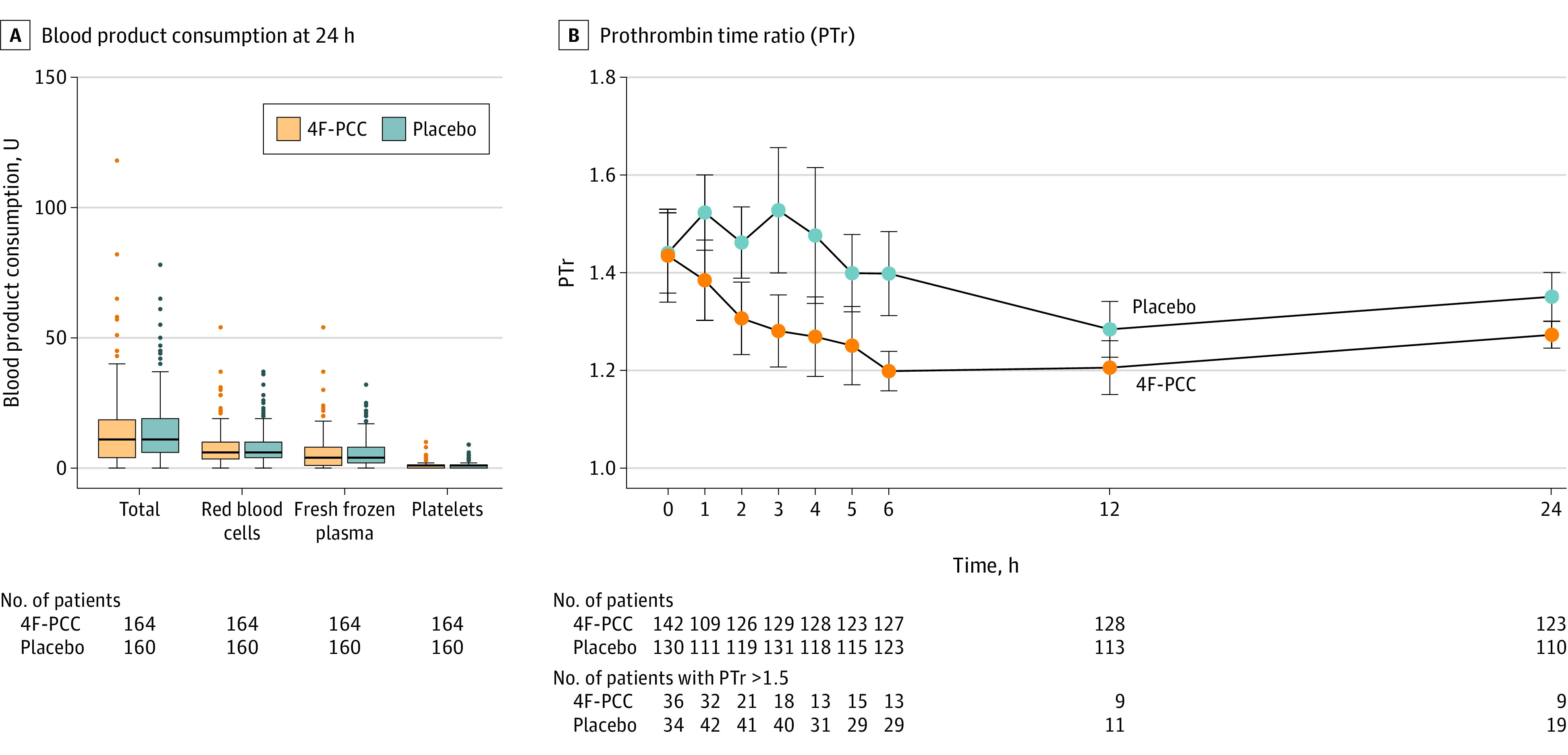
Main outcomes and measures: The primary outcome was 24-hour all blood product consumption (efficacy); arterial or venous thromboembolic events were a secondary outcome (safety).
Results: Of 4313 patients with the highest trauma level activation, 350 were eligible for emergency inclusion, 327 were randomized, and 324 were analyzed (164 in the 4F-PCC group and 160 in the placebo group). The median (IQR) age of participants was 39 (27-56) years, Injury Severity Score was 36 (26-50 [major trauma]), and admission blood lactate level was 4.6 (2.8-7.4) mmol/L; prehospital arterial systolic blood pressure was less than 90 mm Hg in 179 of 324 patients (59%), 233 patients (73%) were men, and 226 (69%) required expedient hemorrhage control. There was no statistically or clinically significant between-group difference in median (IQR) total 24-hour blood product consumption (12 [5-19] U in the 4F-PCC group vs 11 [6-19] U in the placebo group; absolute difference, 0.2 U [95% CI, -2.99 to 3.33]; P = .72). In the 4F-PCC group, 56 patients (35%) presented with at least 1 thromboembolic event vs 37 patients (24%) in the placebo group (absolute difference, 11% [95% CI, 1%-21%]; relative risk, 1.48 [95% CI, 1.04-2.10]; P = .03).
Conclusions and relevance: Among patients with trauma at risk of massive transfusion, there was no significant reduction of 24-hour blood product consumption after administration of 4F-PCC, but thromboembolic events were more common. These findings do not support systematic use of 4F-PCC in patients at risk of massive transfusion.
Trial registration: ClinicalTrials.gov Identifier: NCT03218722.
Conflict of interest statement
Figures

Comment in
-
Four-Factor Prothrombin Complex Concentrate for Patients With Trauma.JAMA. 2023 Sep 5;330(9):875-876. doi: 10.1001/jama.2023.11668. JAMA. 2023. PMID: 37668628 No abstract available.
-
Four-Factor Prothrombin Complex Concentrate for Patients With Trauma.JAMA. 2023 Sep 5;330(9):875. doi: 10.1001/jama.2023.11665. JAMA. 2023. PMID: 37668629 No abstract available.
References
-
- James A, Abback PS, Pasquier P, et al. ; Traumabase Group . The conundrum of the definition of haemorrhagic shock: a pragmatic exploration based on a scoping review, experts’ survey and a cohort analysis. Eur J Trauma Emerg Surg. 2022;48(6):4639-4649. doi: 10.1007/s00068-022-01998-9 - DOI - PMC - PubMed
-
- Crombie N, Doughty HA, Bishop JRB, et al. ; RePHILL collaborative group . Resuscitation with blood products in patients with trauma-related haemorrhagic shock receiving prehospital care (RePHILL): a multicentre, open-label, randomised, controlled, phase 3 trial. Lancet Haematol. 2022;9(4):e250-e261. doi: 10.1016/S2352-3026(22)00040-0 - DOI - PMC - PubMed
