

Best ablation strategy in patients with premature ventricular contractions with multiple morphology: a single-centre experience
- PMID: 36942834
- PMCID: PMC10227647
- DOI: 10.1093/europace/euad038
Best ablation strategy in patients with premature ventricular contractions with multiple morphology: a single-centre experience
Abstract
Aims: This study aimed to examine the clinical benefits of targeted ablation of all Premature ventricular complex (PVC) morphologies vs. predominant PVC only.
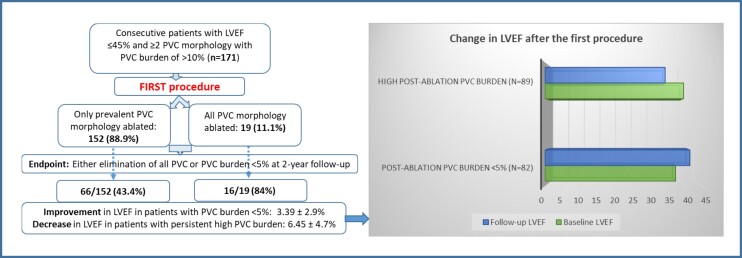
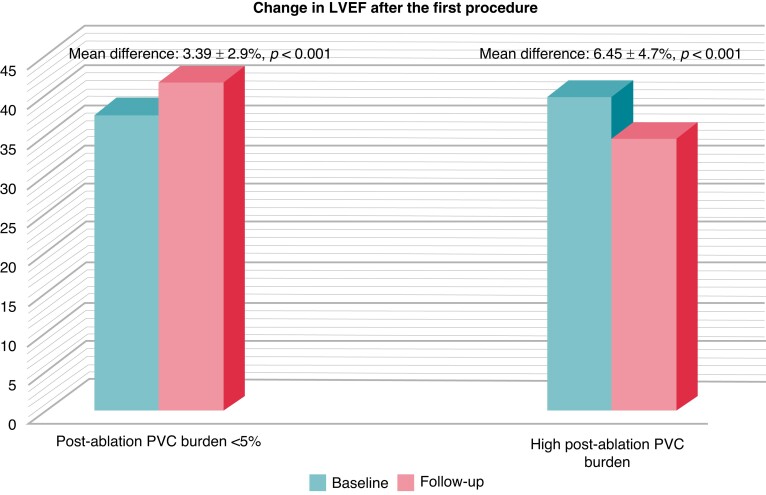
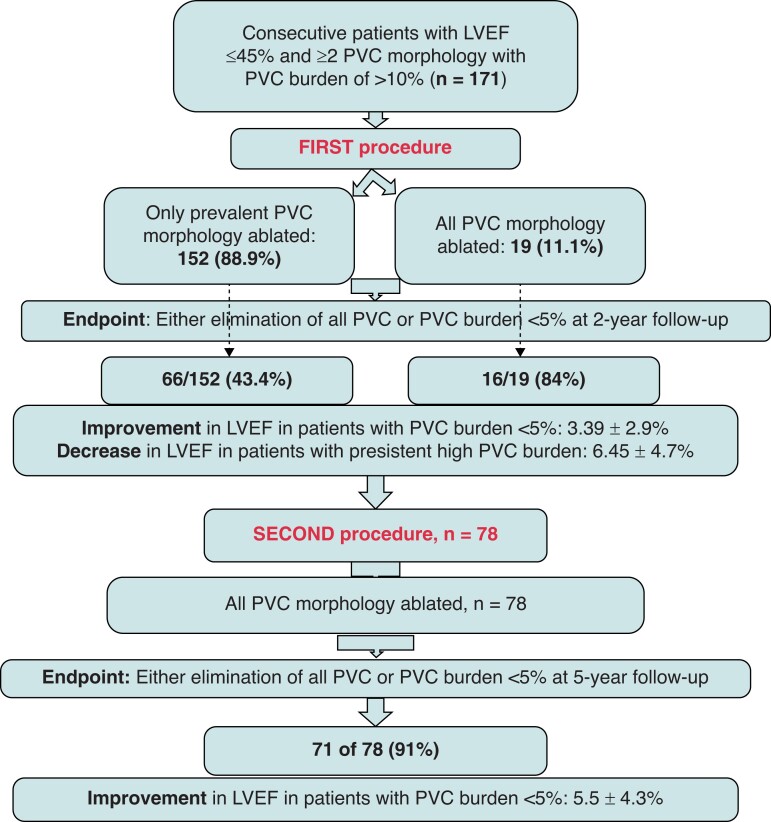
Methods and results: A total of 171 consecutive patients with reduced left ventricular ejection fraction (LVEF) and ≥2 PVC morphology with high burden (>10%/day) undergoing their first ablation procedure were included in the analysis. At the initial procedure, prevalent PVC alone was ablated in the majority. However, at the redo, all PVC morphologies were targeted for ablation. : At the first procedure, 152 (89%) patients received ablation of the dominant PVC only. In the remaining 19 (11%) patients, all PVC morphologies were ablated. At two years, high PVC burden was detected in 89 (52%) patients. Repeat procedure was performed in 78 of 89, where all PVC morphologies were ablated. At 5 years after the repeat procedure, 71 (91%) had PVC burden of <5% [3.8 ± 1.1% vs. 15.4 ± 4.3% in successful vs. failed subjects (P < 0.001)]. In patients with low PVC burden after the initial procedure, LVEF improved from 37.5% to 41.6% [mean difference (MD): 3.39 ± 2.9%, P < 0.001], whereas a reduction in LVEF from 39.8% to 34.5% (MD: 6.45 ± 4.7%, P < 0.001) was recorded in patients with high PVC burden. One year after the repeat procedure, LVEF improved from 36.2% to 41.7% (MD: 5.5 ± 4.3%, P < 0.001) in patients with successful ablation.
Conclusion: In this observational series, ablation of all PVC morphologies was associated with significantly lower PVC burden and improvement of LVEF at long-term follow-up, compared with ablation of the dominant morphology only.
Keywords: LVEF; Morphology; PVC ablation; PVC burden; Premature ventricular complex (PVC).
© The Author(s) 2023. Published by Oxford University Press on behalf of the European Society of Cardiology.
Conflict of interest statement
Conflict of interest: A.N. is a consultant for Abbott, Baylis, Biotronik, Biosense Webster, Boston Scientific, and Medtronic. L.D.B.: Consultant/Advisory Board: Biosense Webster, Hansen Medical, Abbott, Baylis Medical, Biotronik, Boston Scientific, Janssen, Medtronic, Pfizer Inc., Stereotaxis, and Zoll Medical. The other authors have no relevant COI to disclose.
Figures
Comment in
-
Catheter ablation of premature ventricular contractions with multiple morphologies in tachycardia-induced cardiomyopathy: all or nothing?Europace. 2023 May 19;25(5):euad064. doi: 10.1093/europace/euad064. Europace. 2023. PMID: 36942441 Free PMC article. No abstract available.
References
-
- Latchamsetty R, Bogun F. Premature ventricular complexes and premature ventricular Complex induced cardiomyopathy. Curr Probl Cardiol 2015;40:379–422. - PubMed
-
- Bagliani G, Della Rocca DG, De Ponti R, Capucci A, Padeletti M, Natale A. Ectopic beats: insights from timing and morphology. Card Electrophysiol Clin 2018;10:257–75. - PubMed
-
- Latchamsetty R, Yokokawa M, Morady F, Kim HM, Mathew S, Tilz Ret al. . Multicenter outcomes for catheter ablation of idiopathic premature ventricular complexes. JACC Clin Electrophysiol 2015;1:116–23. - PubMed
-
- Sheldon SH, Latchamsetty R, Morady F, Bogun F. Catheter ablation in patients with pleomorphic, idiopathic, premature ventricular complexes. Heart Rhythm 2017;14:1623–8. - PubMed
-
- Zhong L, Lee YH, Huang XM, Asirvatham SJ, Shen WK, Friedman PAet al. . Relative efficacy of catheter ablation vs antiarrhythmic drugs in treating premature ventricular contractions: a single-center retrospective study. Heart Rhythm 2014;11:187–93. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
