

Technology and Tool Development for BACPAC: Qualitative and Quantitative Analysis of Accelerated Lumbar Spine MRI with Deep-Learning Based Image Reconstruction at 3T
- PMID: 36943371
- PMCID: PMC10403300
- DOI: 10.1093/pm/pnad035
Technology and Tool Development for BACPAC: Qualitative and Quantitative Analysis of Accelerated Lumbar Spine MRI with Deep-Learning Based Image Reconstruction at 3T
Abstract
Objectives: To evaluate whether combining fast acquisitions with deep-learning reconstruction can provide diagnostically useful images and quantitative assessment comparable to standard-of-care acquisitions for lumbar spine magnetic resonance imaging (MRI).
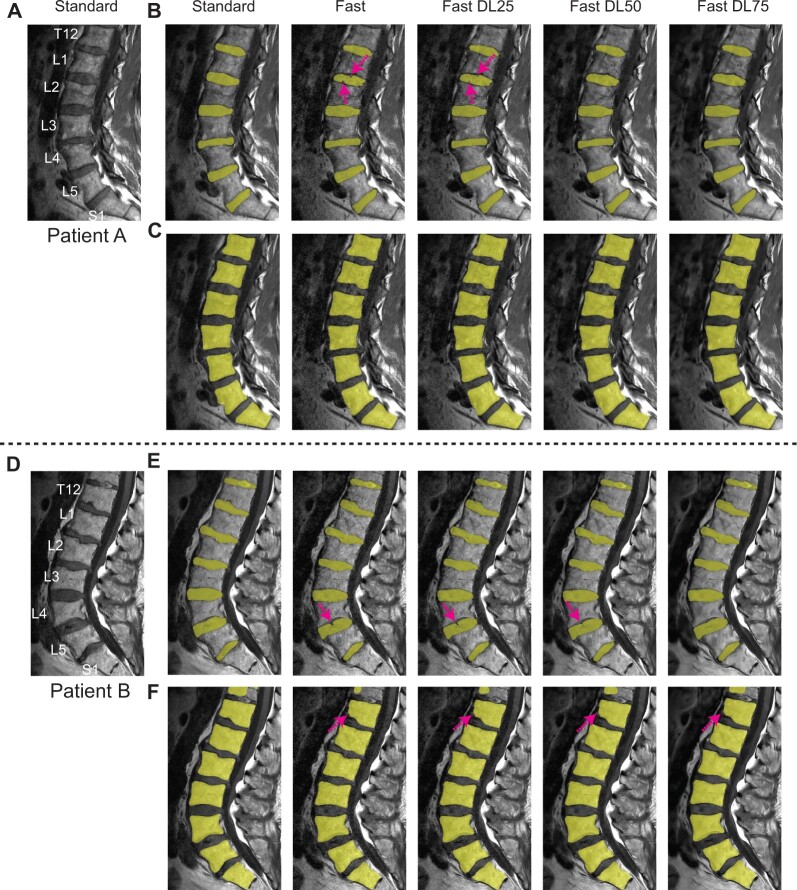
Methods: Eighteen patients were imaged with both standard protocol and fast protocol using reduced signal averages, each protocol including sagittal fat-suppressed T2-weighted, sagittal T1-weighted, and axial T2-weighted 2D fast spin-echo sequences. Fast-acquisition data was additionally reconstructed using vendor-supplied deep-learning reconstruction with three different noise reduction factors. For qualitative analysis, standard images as well as fast images with and without deep-learning reconstruction were graded by three radiologists on five different categories. For quantitative analysis, convolutional neural networks were applied to sagittal T1-weighted images to segment intervertebral discs and vertebral bodies, and disc heights and vertebral body volumes were derived.
Results: Based on noninferiority testing on qualitative scores, fast images without deep-learning reconstruction were inferior to standard images for most categories. However, deep-learning reconstruction improved the average scores, and noninferiority was observed over 24 out of 45 comparisons (all with sagittal T2-weighted images while 4/5 comparisons with sagittal T1-weighted and axial T2-weighted images). Interobserver variability increased with 50 and 75% noise reduction factors. Deep-learning reconstructed fast images with 50% and 75% noise reduction factors had comparable disc heights and vertebral body volumes to standard images (r2≥ 0.86 for disc heights and r2≥ 0.98 for vertebral body volumes).
Conclusions: This study demonstrated that deep-learning-reconstructed fast-acquisition images have the potential to provide noninferior image quality and comparable quantitative assessment to standard clinical images.
Keywords: clinical MRI; deep learning reconstruction; fast acquisition; lower back pain; lumbar spine MRI; segmentation.
© The Author(s) 2023. Published by Oxford University Press on behalf of the American Academy of Pain Medicine.
Figures





References
-
- Hoy D, March L, Brooks P, et al.Measuring the global burden of low back pain. Best Pract Res Clin Rheumatol. 2010;24(2):155–165. - PubMed
-
- Dagenais S, Caro J, Haldeman S.. A systematic review of low back pain cost of illness studies in the United States and internationally. Spine J. 2008;8(1):8–20. - PubMed
-
- Luo X, Pietrobon R, Sun SX, Liu GG, Hey L.. Estimates and patterns of direct health care expenditures among individuals with back pain in the United States. Spine (Phila Pa 1976). 2004;29(1):79–86. - PubMed
