

Apical Ischemia Is a Universal Feature of Apical Hypertrophic Cardiomyopathy
- PMID: 36943913
- PMCID: PMC10026964
- DOI: 10.1161/CIRCIMAGING.122.014907
Apical Ischemia Is a Universal Feature of Apical Hypertrophic Cardiomyopathy
Abstract
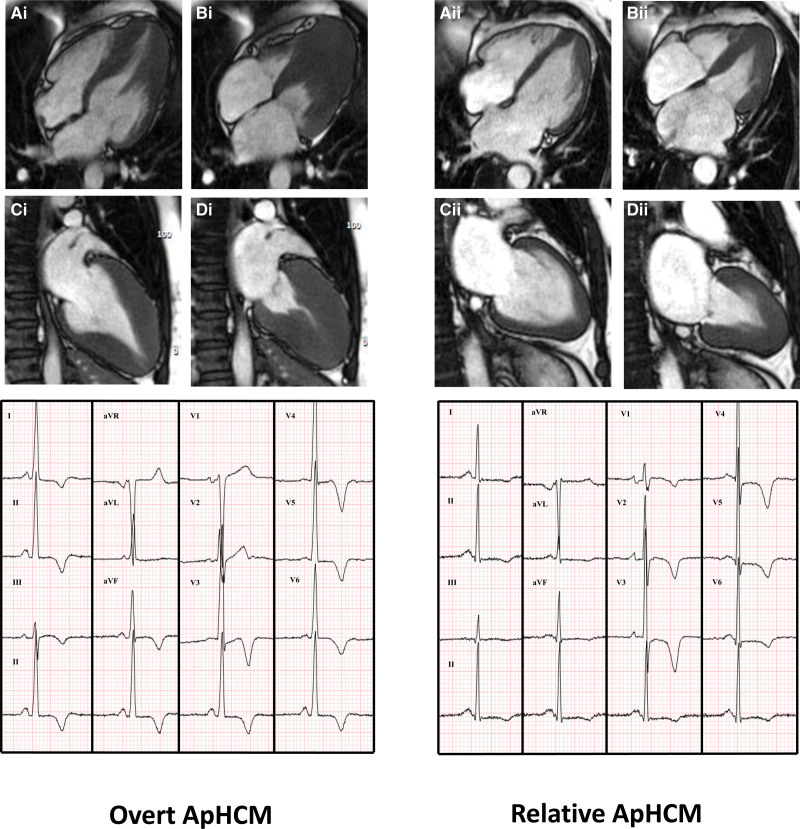
Background: Apical hypertrophic cardiomyopathy (ApHCM) accounts for ≈10% of hypertrophic cardiomyopathy cases and is characterized by apical hypertrophy, apical cavity obliteration, and tall ECG R waves with ischemic-looking deep T-wave inversion. These may be present even with <15 mm apical hypertrophy (relative ApHCM). Microvascular dysfunction is well described in hypertrophic cardiomyopathy. We hypothesized that apical perfusion defects would be common in ApHCM.
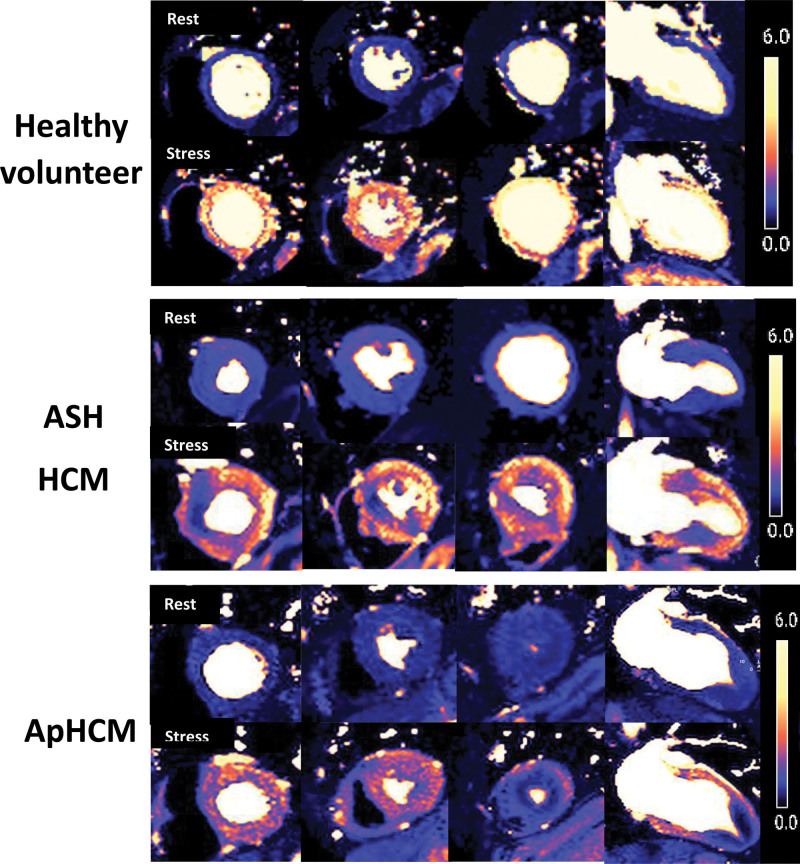
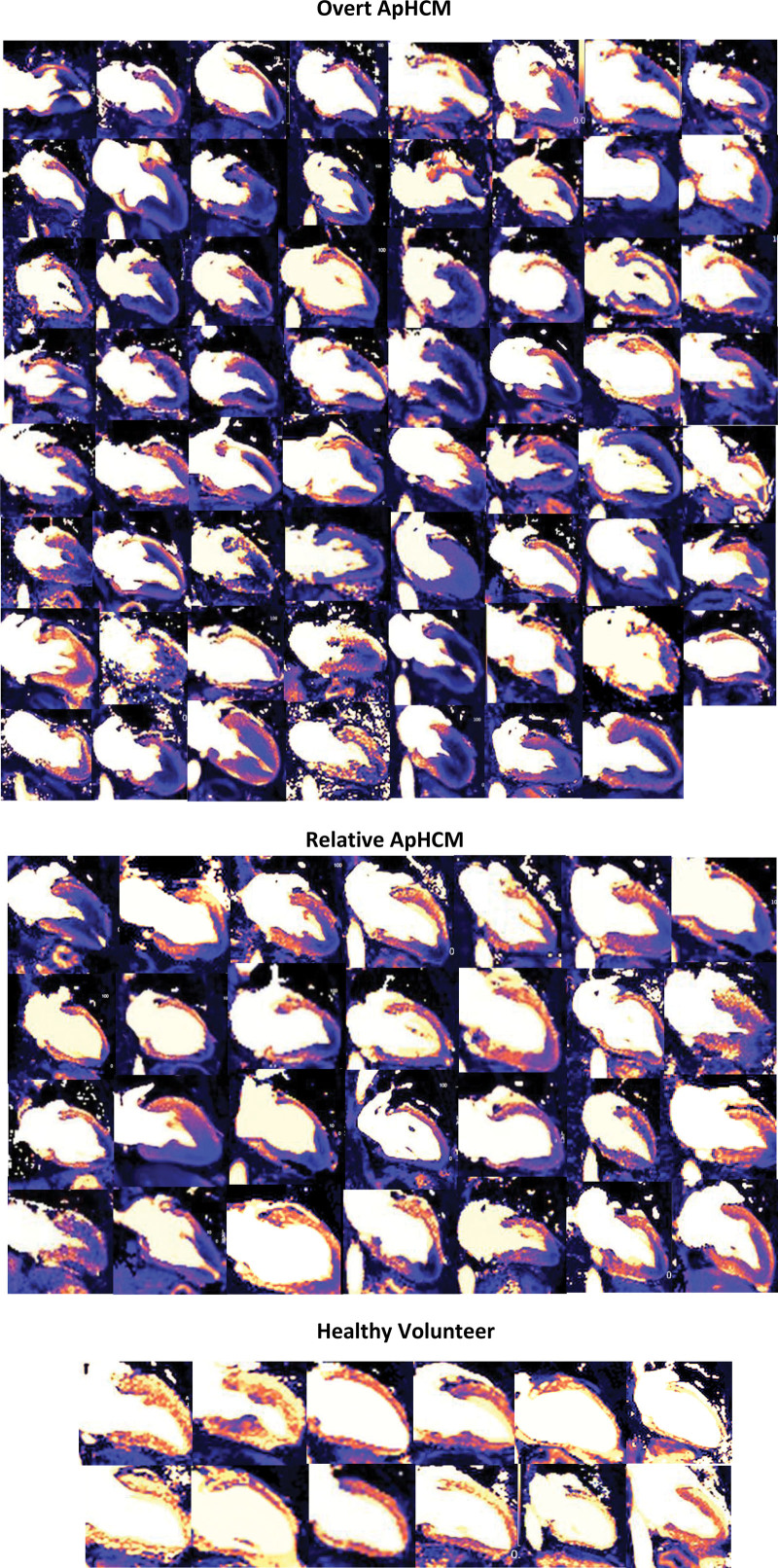
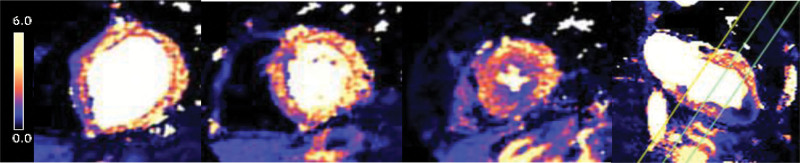
Methods: A 2-center study using cardiovascular magnetic resonance short- and long-axis quantitative adenosine vasodilator stress perfusion mapping. One hundred patients with ApHCM (68 overt hypertrophy [≥15 mm] and 32 relative ApHCM) were compared with 50 patients with asymmetrical septal hypertrophy hypertrophic cardiomyopathy and 40 healthy volunteer controls. Perfusion was assessed visually and quantitatively as myocardial blood flow and myocardial perfusion reserve.
Results: Apical perfusion defects were present in all overt ApHCM patients (100%), all relative ApHCM patients (100%), 36% of asymmetrical septal hypertrophy hypertrophic cardiomyopathy, and 0% of healthy volunteers (P<0.001). In 10% of patients with ApHCM, perfusion defects were sufficiently apical that conventional short-axis views missed them. In 29%, stress myocardial blood flow fell below rest values. Stress myocardial blood flow was most impaired subendocardially, with greater hypertrophy or scar, and with apical aneurysms. Impaired apical myocardial blood flow was most strongly predicted by thicker apical segments (β-coefficient, -0.031 mL/g per min [CI, -0.06 to -0.01]; P=0.013), higher ejection fraction (-0.025 mL/g per min [CI, -0.04 to -0.01]; P<0.005), and ECG maximum R-wave height (-0.023 mL/g per min [CI, -0.04 to -0.01]; P<0.005).
Conclusions: Apical perfusion defects are universally present in ApHCM at all stages. Its ubiquitous presence along with characteristic ECG suggests ischemia may play a disease-defining role in ApHCM.
Keywords: apical hypertrophic cardiomyopathy; cardiomyopathy; humans; hypertrophic; hypertrophy; stroke volume.
Conflict of interest statement
None.
Figures
References
-
- Ommen SR, Mital S, Burke MA, Day SM, Deswal A, Elliott P, Evanovich LL, Hung J, Joglar JA, Kantor P, et al. . 2020 AHA/ACC guideline for the diagnosis and treatment of patients with hypertrophic cardiomyopathy. Circulation. 2020;142:e558–e631. doi: 10.1161/CIR.0000000000000937 - PubMed
-
- Elliott PM, Anastasakis A, Borger M, Borggrefe M, Cecchi F, Charron P, Hagege A, Lafont A. 2014 ESC guidelines on diagnosis and management of hypertrophic cardiomyopathy. Eur Heart J. 2014;35:2733–2779. doi: 10.1093/eurheartj/ehu284 - PubMed
-
- Klarich KW, Jost CHA, Binder J, Connolly HM, Scott CG, Freeman WK, Ackerman MJ, Nishimura RA, Tajik AJ, Ommen SR. Risk of death in long-term follow-up of patients with apical hypertrophic cardiomyopathy. Am J Cardiol. 2013;111:1784–1791. doi: 10.1016/j.amjcard.2013.02.040 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
