

Novel Prognostic Staging System for Patients With De Novo Metastatic Breast Cancer
- PMID: 36944149
- PMCID: PMC10414698
- DOI: 10.1200/JCO.22.02222
Novel Prognostic Staging System for Patients With De Novo Metastatic Breast Cancer
Abstract
Purpose: Given the heterogeneity and improvement in outcomes for metastatic breast cancer (MBC), we developed a staging system that refines prognostic estimates for patients with metastatic cancer at the time of initial diagnosis, de novo MBC (dnMBC), on the basis of survival outcomes and disease-related variables.
Methods: Patients with dnMBC (2010-2016) were selected from the National Cancer Database (NCDB). Recursive partitioning analysis (RPA) was used to group patients with similar overall survival (OS) on the basis of clinical T category, grade, estrogen receptor (ER), progesterone receptor, human epidermal growth factor receptor 2, histology, organ system site of metastases (bone-only, brain-only, visceral), and number of organ systems involved. Three-year OS rates were used to assign a final stage: IVA: >70%, IVB: 50%-70%, IVC: 25 to <50%, and IVD: <25%. Bootstrapping was applied with 1,000 iterations, and final stage assignments were made based on the most commonly occurring assignment. Unadjusted OS was estimated. Validation analyses were conducted using SEER and NCDB.
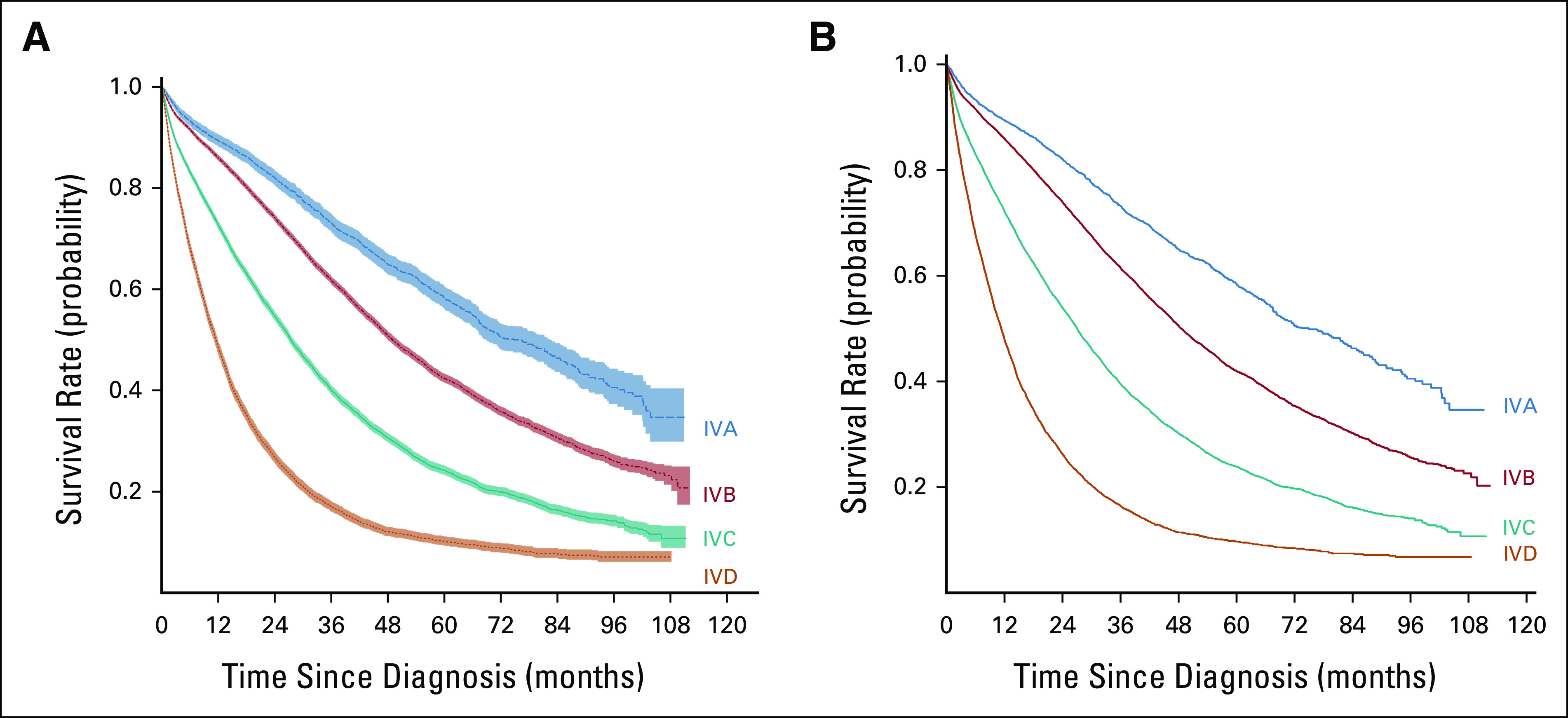
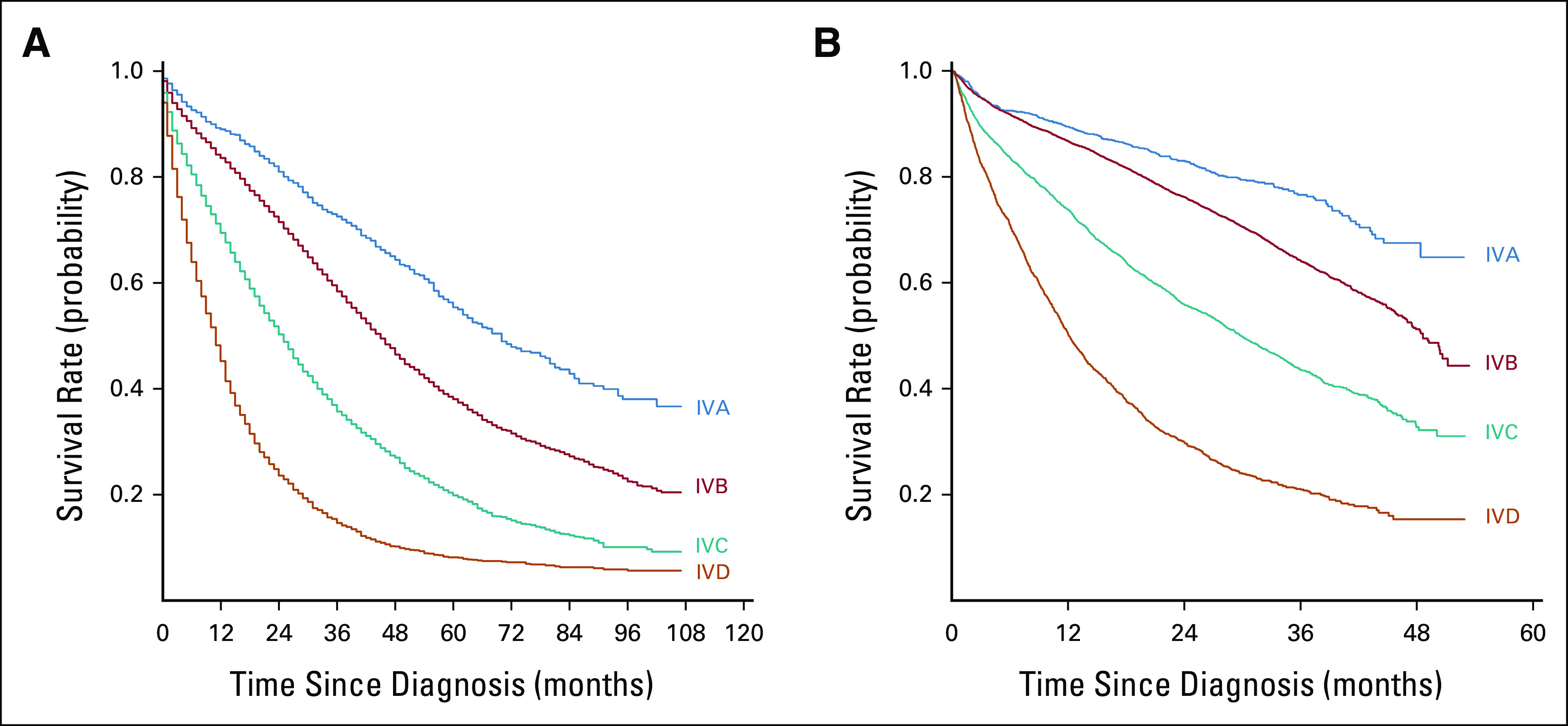
Results: At a median follow-up of 52.9 months, the median OS of the original cohort (N = 42,467) was 35.4 months (95% CI, 34.8 to 35.9). RPA stratified patients into 53 groups with 3-year OS rates ranging from 73.5% to 5.7%; these groups were amalgamated into four stage groups: 3-year OS, A = 73.2%, B = 61.9%, C = 40.1%, and D = 17% (log-rank P < .001). After bootstrapping, the survival outcomes for the four stages remained significantly different (log-rank P < .001). This staging system was then validated using SEER data (N = 20,469) and a separate cohort from the NCDB (N = 7,645) (both log-rank P < .001).
Conclusion: Our findings regarding the heterogeneity in outcomes for patients with dnMBC could guide future revisions of the current American Joint Committee on Cancer staging guidelines for patients with newly diagnosed stage IV disease. Our findings should be independently confirmed.
Conflict of interest statement
The following represents disclosure information provided by authors of this manuscript. All relationships are considered compensated unless otherwise noted. Relationships are self-held unless noted. I = Immediate Family Member, Inst = My Institution. Relationships may not relate to the subject matter of this manuscript. For more information about ASCO's conflict of interest policy, please refer to
Open Payments is a public database containing information reported by companies about payments made to US-licensed physicians (
No other potential conflicts of interest were reported.
Figures
References
-
- Surveillance, Epidemiology, and End Results (SEER): Cancer Stat Facts : Female Breast Cancer. Bethesda, MD, National Cancer Institute, 2022
-
- Clark GM, Sledge GW Jr., Osborne CK, et al. : Survival from first recurrence: Relative importance of prognostic factors in 1,015 breast cancer patients. J Clin Oncol 5:55-61, 1987 - PubMed
-
- Yamamoto N, Watanabe T, Katsumata N, et al. : Construction and validation of a practical prognostic index for patients with metastatic breast cancer. J Clin Oncol 16:2401-2408, 1998 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
