

Anthropometric measures and adverse outcomes in heart failure with reduced ejection fraction: revisiting the obesity paradox
- PMID: 36944496
- PMCID: PMC10111968
- DOI: 10.1093/eurheartj/ehad083
Anthropometric measures and adverse outcomes in heart failure with reduced ejection fraction: revisiting the obesity paradox
Abstract
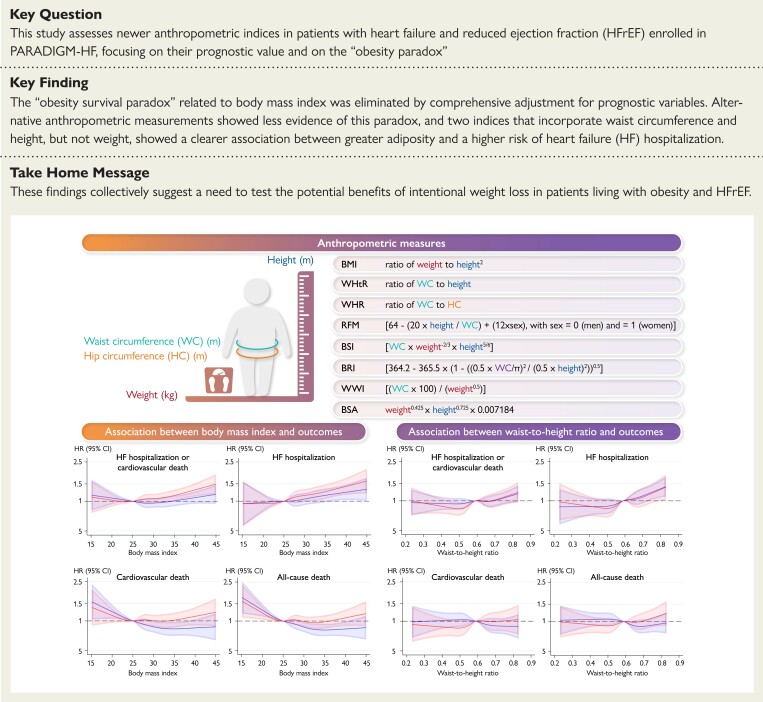
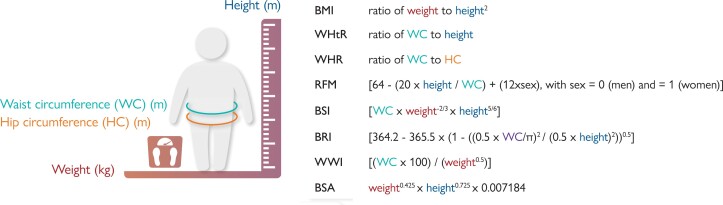
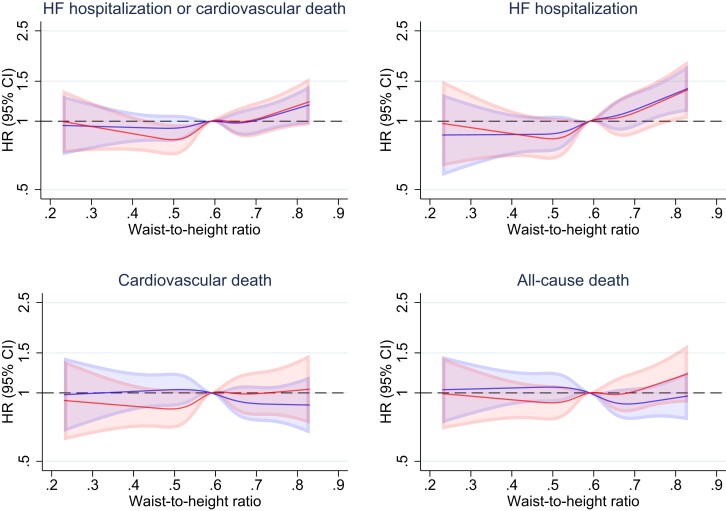
Aims: Although body mass index (BMI) is the most commonly used anthropometric measure, newer indices such as the waist-to-height ratio, better reflect the location and amount of ectopic fat, as well as the weight of the skeleton, and may be more useful.
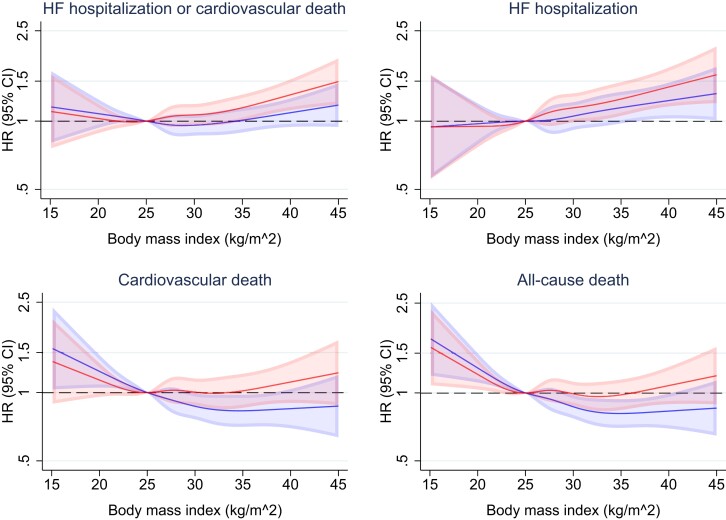
Methods and results: The prognostic value of several newer anthropometric indices was compared with that of BMI in patients with heart failure (HF) and reduced ejection fraction (HFrEF) enrolled in prospective comparison of ARNI with ACEI to determine impact on global mortality and morbidity in heart failure. The primary outcome was HF hospitalization or cardiovascular death. The association between anthropometric indices and outcomes were comprehensively adjusted for other prognostic variables, including natriuretic peptides. An 'obesity-survival paradox' related to lower mortality risk in those with BMI ≥25 kg/m2 (compared with normal weight) was identified but this was eliminated by adjustment for other prognostic variables. This paradox was less evident for waist-to-height ratio (as an exemplar of indices not incorporating weight) and eliminated by adjustment: the adjusted hazard ratio (aHR) for all-cause mortality, for quintile 5 vs. quintile 1, was 1.10 [95% confidence interval (CI) 0.87-1.39]. However, both BMI and waist-to-height ratio showed that greater adiposity was associated with a higher risk of the primary outcome and HF hospitalization; this was more evident for waist-to-height ratio and persisted after adjustment e.g. the aHR for HF hospitalization for quintile 5 vs. quintile 1 of waist-to-height ratio was 1.39 (95% CI 1.06-1.81).
Conclusion: In patients with HFrEF, alternative anthropometric measurements showed no evidence for an 'obesity-survival paradox'. Newer indices that do not incorporate weight showed that greater adiposity was clearly associated with a higher risk of HF hospitalization.
Keywords: Angiotensin receptor-neprilysin inhibitor; Body mass index; Clinical trial; Heart failure with reduced ejection fraction; Obesity.
© The Author(s) 2023. Published by Oxford University Press on behalf of the European Society of Cardiology. All rights reserved. For permissions, please e-mail: journals.permissions@oup.com.
Conflict of interest statement
Conflict of interest: Dr. Butt reports advisory board honoraria from Bayer. Dr. Petrie has received research grants or consultancy fees from SQ Innovations, AstraZeneca, Roche, Boehringer Ingelheim, Pharmacosmos, Eli Lilly, Napp Pharmaceuticals, Novartis, and Novo Nordisk and has served on clinical events committees for AbbVie, Alnylam, AstraZeneca, Bayer, Boehringer Ingelheim, GlaxoSmithKline, Resverlogix, and Novo Nordisk. Dr. Jhund has received consulting fees, advisory board fees, and lecture fees from Novartis; advisory board fees from Cytokinetics; and grant support from Boehringer Ingelheim. Dr. Sattar has consulted for or received lecture fees from Afimmune, Amgen, AstraZeneca, Boehringer Ingelheim, Eli Lilly, Hanmi Pharmaceuticals, Merck Sharp & Dohme, Novartis, Novo Nordisk, Pfizer, and Sanofi. He has received grant support from AstraZeneca, Boehringer Ingelheim, Novartis, and Roche Diagnostics through his institution, the University of Glasgow. Dr. Desai reported receiving personal fees from Abbott, Biofourmis, Boston Scientific, Boehringer Ingelheim, Merck, Regeneron, and Relypsa and grants and personal fees from AstraZeneca, Alnylam, and Novartis outside the submitted work. Dr. Kober reports personal fees from speaker honoraria from Novartis, AstraZeneca, Novo Nordisk, and Boehringer Ingelheim. Dr. Rouleau has received grants and consulting fees from Novartis and consulting fees from Abbott, AstraZeneca, MyoKardia, and Sanofi. Dr. Swedberg reports honoraria from AstraZeneca, Boehringer 12 Ingelheim, and Novartis. Dr. Zile has received research funding from Novartis and has been a consultant for Novartis, Abbott, Boston Scientific, CVRx, EBR, Endotronics, Ironwood, Merck, Medtronic, and Myokardia V Wave. Dr. Solomon has received research grants from Actelion, Alnylam, Amgen, AstraZeneca, Bellerophon, Bayer, BMS, Celladon, Cytokinetics, Eidos, Gilead, GSK, Ionis, Lilly, Lone Star Heart, Mesoblast, MyoKardia, NIH/NHLBI, Neurotronik, Novartis, NovoNordisk, Respicardia, Sanofi Pasteur, Theracos, and has consulted for Abbott, Action Akros, Alnylam, Amgen, Arena, AstraZeneca, Bayer, Boeringer-Ingelheim, BMS, Cardior, Cardurion, Corvia, Cytokinetics, Daiichi-Sankyo, Gilead, GSK, Ironwood, Lilly, Merck, Myokardia, Novartis, Roche, Takeda, Theracos, Quantum Genetics, Cardurion, AoBiome, Janssen, Cardiac Dimensions, Tenaya, Sanofi-Pasteur, Dinaqor, Tremeau, CellProThera, Moderna, and American Regent. Dr. Packer has received consulting fees from AbbVie, Akcea, Actavis, Amgen, AstraZeneca, Bayer, Boehringer Ingelheim, Cardiorentis, Daiichi Sankyo, Gilead, Johnson & Johnson, Novo Nordisk, Pfizer, Relypsa, Sanofi, Synthetic Biologics, and Theravance. Dr. McMurray reports payments to his employer, Glasgow University, for work on clinical trials, consulting, lecturing and other activities: Alnylam, Amgen, AstraZeneca, Bayer, Boehringer Ingelheim, BMS, Cardurion, Cytokinetics, Dal-Cor, GSK, Ionis, KBP Biosciences, Novartis, Pfizer, and Theracos. Personal lecture fees: Abbott, Hikma, Sun Pharmaceuticals, Servier, Theracos; and personal payments from Abbott, Hikma, Ionis, Sun Pharmaceuticals, Servier. The other authors report no conflicts.
Figures
Comment in
-
Revisiting the obesity paradox in heart failure: what is the best anthropometric index to gauge obesity?Eur Heart J. 2023 Apr 1;44(13):1154-1156. doi: 10.1093/eurheartj/ehad079. Eur Heart J. 2023. PMID: 36944505 No abstract available.
-
Waist-to-height ratio for the obesity paradox in heart failure: is it a matter of fitness?Eur Heart J. 2023 Sep 14;44(35):3386-3387. doi: 10.1093/eurheartj/ehad503. Eur Heart J. 2023. PMID: 37529967 No abstract available.
References
-
- Aune D, Sen A, Norat T, Janszky I, Romundstad P, Tonstad S, et al. . Body mass index, abdominal fatness, and heart failure incidence and mortality: a systematic review and dose-response meta-analysis of prospective studies. Circulation 2016;133:639–649. 10.1161/CIRCULATIONAHA.115.016801 - DOI - PubMed
-
- Zhang J, Begley A, Jackson R, Harrison M, Pellicori P, Clark AL, et al. . Body mass index and all-cause mortality in heart failure patients with normal and reduced ventricular ejection fraction: a dose–response meta-analysis. Clin Res Cardiol 2019;108:119–132. 10.1007/s00392-018-1302-7 - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
