

Clinical evidence for immune-based strategies in early-line multiple myeloma: current challenges in decision-making for subsequent therapy
- PMID: 36944635
- PMCID: PMC10030780
- DOI: 10.1038/s41408-023-00804-y
Clinical evidence for immune-based strategies in early-line multiple myeloma: current challenges in decision-making for subsequent therapy
Erratum in
-
Correction: Clinical evidence for immune-based strategies in early-line multiple myeloma: current challenges in decision-making for subsequent therapy.Blood Cancer J. 2023 Jul 6;13(1):104. doi: 10.1038/s41408-023-00866-y. Blood Cancer J. 2023. PMID: 37407575 Free PMC article. No abstract available.
Abstract
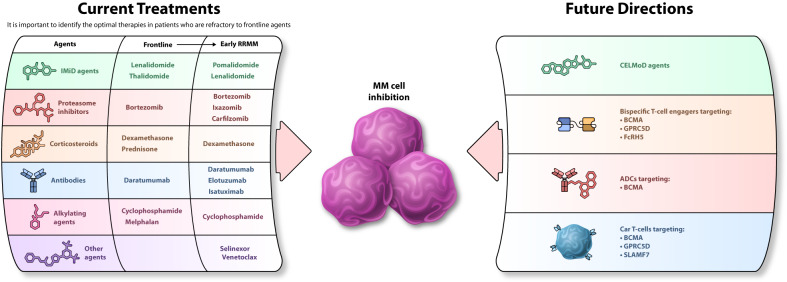
Almost all patients with multiple myeloma (MM) will eventually develop disease that has relapsed with or become refractory to available treatments and will require additional therapy. However, data are still lacking on how best to sequence regimens in the relapsed/refractory (RR) setting after the failure of early-line lenalidomide, bortezomib, and/or daratumumab, the most commonly used agents in clinical practice today. With the treatment landscape rapidly changing in response to emerging clinical trial data and approvals of several new drugs and additional combinations, it is critically important to focus on patients with RRMM. Variability in patient baseline characteristics, such as the number of prior lines of treatment, refractoriness to prior treatments, prior stem cell transplant, and timing and dosing of prior lenalidomide, makes it difficult to select the best options for patients with RRMM for whom first-line treatments have failed. The aim of this review is to provide both an overview of current therapies and future directions within the RRMM treatment landscape, and a framework for clinicians to choose the most promising next treatment option.
© 2023. The Author(s).
Conflict of interest statement
NR reports consulting for Amgen, Bristol Myers Squibb, Janssen, Sanofi, Takeda, AstraZeneca, and C4 Therapeutics, and serving on the advisory boards of Caribou and Immuneel, and research funding from bluebird bio; M-VM reports payment or honoraria from Janssen, Bristol Myers Squibb, Amgen, Takeda, GlaxoSmithKline, Sanofi, Regeneron, Pfizer, and Seagen; SL reports receiving support for the present manuscript from Bristol Myers Squibb, and grant or contract support from Bristol Myers Squibb, Janssen, Sanofi, Pfizer, AbbVie, Daiichi Sankyo, Takeda, Ono, Chugai, Amgen, GlaxoSmithKline, and Kyowa Kirin, and payments or honoraria from Bristol Myers Squibb, Janssen, Takeda, Ono, Pfizer, Sanofi, and Celgene; DR reports consulting fees from Janssen, Bristol Myers Squibb, Amgen, and Takeda, and payment or honoraria from Janssen, Bristol Myers Squibb, Amgen, Takeda, and Merck, and research funding from Janssen, Bristol Myers Squibb, Amgen, Otsuka, Merck, and Takeda, and serving on the board of directors or advisory committees for Janssen and Bristol Myers Squibb.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
