

Non-invasive measurements of ictal and interictal epileptiform activity using optically pumped magnetometers
- PMID: 36944674
- PMCID: PMC10030968
- DOI: 10.1038/s41598-023-31111-y
Non-invasive measurements of ictal and interictal epileptiform activity using optically pumped magnetometers
Abstract
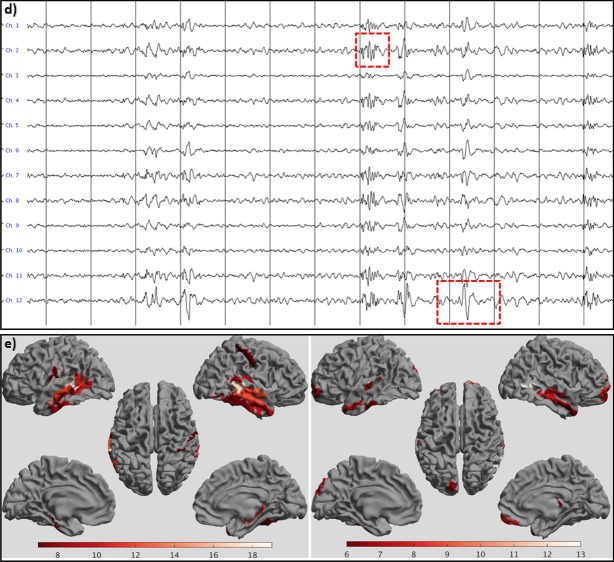
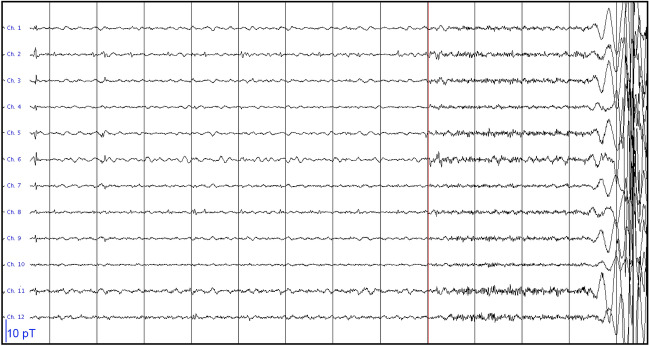
Magneto- and electroencephalography (MEG/EEG) are important techniques for the diagnosis and pre-surgical evaluation of epilepsy. Yet, in current cryogen-based MEG systems the sensors are offset from the scalp, which limits the signal-to-noise ratio (SNR) and thereby the sensitivity to activity from deep structures such as the hippocampus. This effect is amplified in children, for whom adult-sized fixed-helmet systems are typically too big. Moreover, ictal recordings with fixed-helmet systems are problematic because of limited movement tolerance and/or logistical considerations. Optically Pumped Magnetometers (OPMs) can be placed directly on the scalp, thereby improving SNR and enabling recordings during seizures. We aimed to demonstrate the performance of OPMs in a clinical population. Seven patients with challenging cases of epilepsy underwent MEG recordings using a 12-channel OPM-system and a 306-channel cryogen-based whole-head system: three adults with known deep or weak (low SNR) sources of interictal epileptiform discharges (IEDs), along with three children with focal epilepsy and one adult with frequent seizures. The consistency of the recorded IEDs across the two systems was assessed. In one patient the OPMs detected IEDs that were not found with the SQUID-system, and in two patients no IEDs were found with either system. For the other patients the OPM data were remarkably consistent with the data from the cryogenic system, noting that these were recorded in different sessions, with comparable SNRs and IED-yields overall. Importantly, the wearability of OPMs enabled the recording of seizure activity in a patient with hyperkinetic movements during the seizure. The observed ictal onset and semiology were in agreement with previous video- and stereo-EEG recordings. The relatively affordable technology, in combination with reduced running and maintenance costs, means that OPM-based MEG could be used more widely than current MEG systems, and may become an affordable alternative to scalp EEG, with the potential benefits of increased spatial accuracy, reduced sensitivity to volume conduction/field spread, and increased sensitivity to deep sources. Wearable MEG thus provides an unprecedented opportunity for epilepsy, and given its patient-friendliness, we envisage that it will not only be used for presurgical evaluation of epilepsy patients, but also for diagnosis after a first seizure.
© 2023. The Author(s).
Conflict of interest statement
M.J.B. is a director of Cerca Magnetics Limited, a spin-out company whose aim is to commercialise aspects of OPM-MEG technology. Cerca products include bi-planar coils such as those used in this work. N.H., M.J.B. and R.B. hold founding equity in Cerca Magnetics Limited, and N.H. and R.B. sit on the scientific advisory board. All other authors have no conflict of interest.
Figures
References
-
- Lüders HO, Najm I, Nair D, Widdess-Walsh P, Bingman W. The epileptogenic zone: General principles. Epileptic Disord. 2006;8(Suppl 2):S1–S9. - PubMed
