

CytoSorb hemoperfusion markedly attenuates circulating cytokine concentrations during systemic inflammation in humans in vivo
- PMID: 36945034
- PMCID: PMC10029173
- DOI: 10.1186/s13054-023-04391-z
CytoSorb hemoperfusion markedly attenuates circulating cytokine concentrations during systemic inflammation in humans in vivo
Abstract
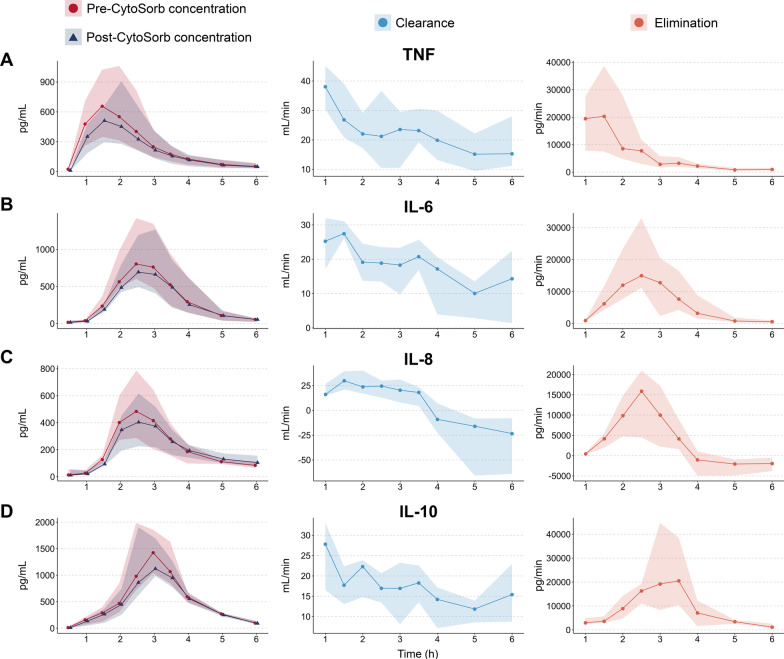
Background: The CytoSorb hemoadsorption device has been demonstrated to be capable of clearing inflammatory cytokines, but has not yet been shown to attenuate plasma cytokine concentrations. We investigated the effects of CytoSorb hemoperfusion on plasma levels of various cytokines using the repeated human experimental endotoxemia model, a highly standardized and reproducible human in vivo model of systemic inflammation and immunological tolerance induced by administration of bacterial lipopolysaccharide (LPS).
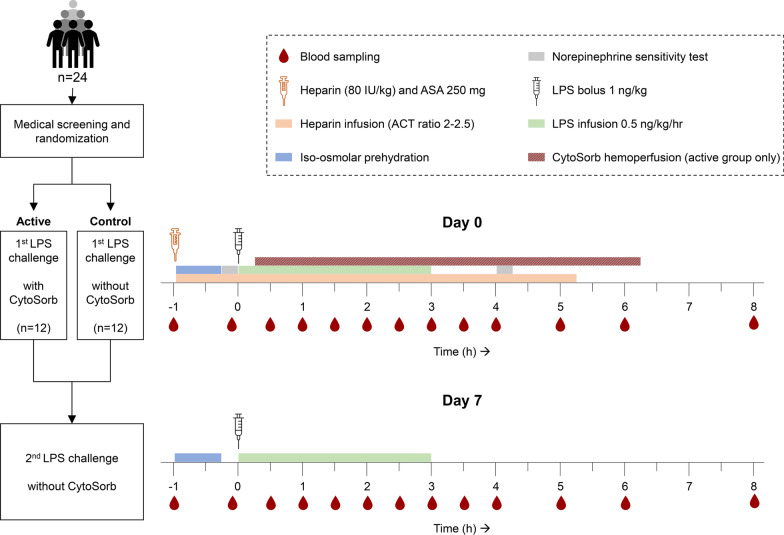
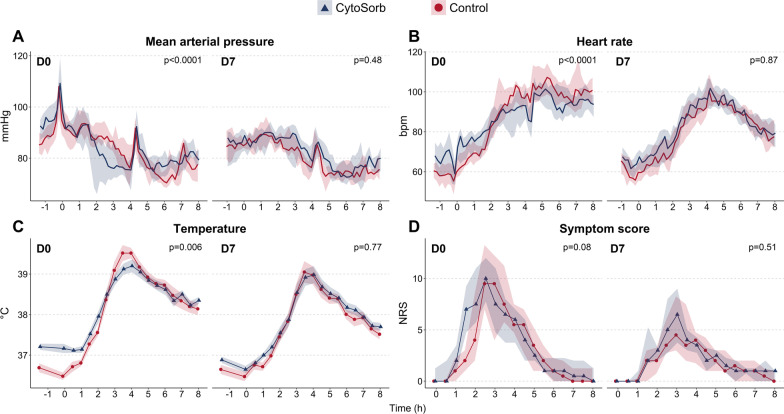
Methods: Twenty-four healthy male volunteers (age 18-35) were intravenously challenged with LPS (a bolus of 1 ng/kg followed by continuous infusion of 0.5 ng/kg/hr for three hours) twice: on day 0 to quantify the initial cytokine response and on day 7 to quantify the degree of endotoxin tolerance. Subjects either received CytoSorb hemoperfusion during the first LPS challenge (CytoSorb group), or no intervention (control group). Plasma cytokine concentrations and clearance rates were determined serially. This study was registered at ClinicalTrials.gov (NCT04643639, date of registration November 24th 2020).
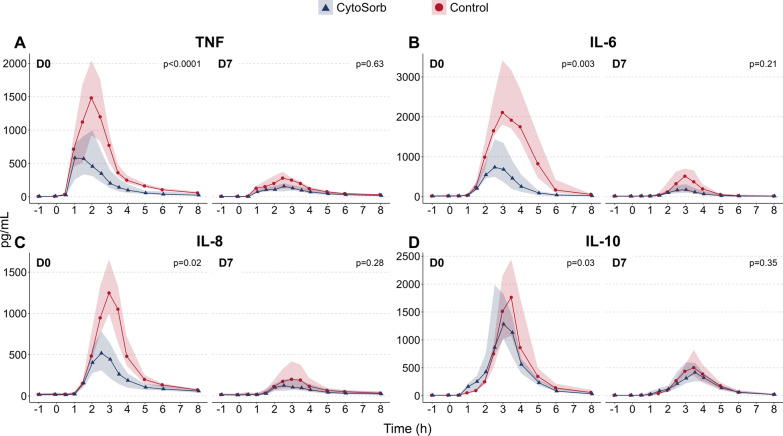
Results: LPS administration led to a profound increase in plasma cytokine concentrations during both LPS challenge days. Compared to the control group, significantly lower plasma levels of tumor necrosis factor (TNF, - 58%, p < 0.0001), interleukin (IL)-6 ( - 71%, p = 0.003), IL-8 ( - 48%, p = 0.02) and IL-10 ( - 26%, p = 0.03) were observed in the CytoSorb group during the first LPS challenge. No differences in cytokine responses were observed during the second LPS challenge.
Conclusions: CytoSorb hemoperfusion effectively attenuates circulating cytokine concentrations during systemic inflammation in humans in vivo, whereas it does not affect long-term immune function. Therefore, CytoSorb therapy may be of benefit in conditions characterized by excessive cytokine release.
Keywords: CytoSorb; Cytokines; Extracorporeal therapy; Hemoadsorption; Sepsis; Systemic inflammation.
© 2023. The Author(s).
Conflict of interest statement
The authors have no competing interest to declare.
Figures
Comment in
-
The phenomenon of desorption: What are the best adsorber exchange intervals?Crit Care. 2024 May 27;28(1):178. doi: 10.1186/s13054-024-04968-2. Crit Care. 2024. PMID: 38802971 Free PMC article. No abstract available.
-
Desorption in hemoadsorption therapies: a call for more data.Crit Care. 2024 Jun 24;28(1):207. doi: 10.1186/s13054-024-04995-z. Crit Care. 2024. PMID: 38915114 Free PMC article. No abstract available.
References
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
