

This is a preprint.
Noninvasive electrophysiological imaging identifies 4D uterine peristalsis patterns in subjects with normal menstrual cycles and patients with endometriosis
- PMID: 36945376
- PMCID: PMC10029120
- DOI: 10.21203/rs.3.rs-2432192/v1
Noninvasive electrophysiological imaging identifies 4D uterine peristalsis patterns in subjects with normal menstrual cycles and patients with endometriosis
Abstract
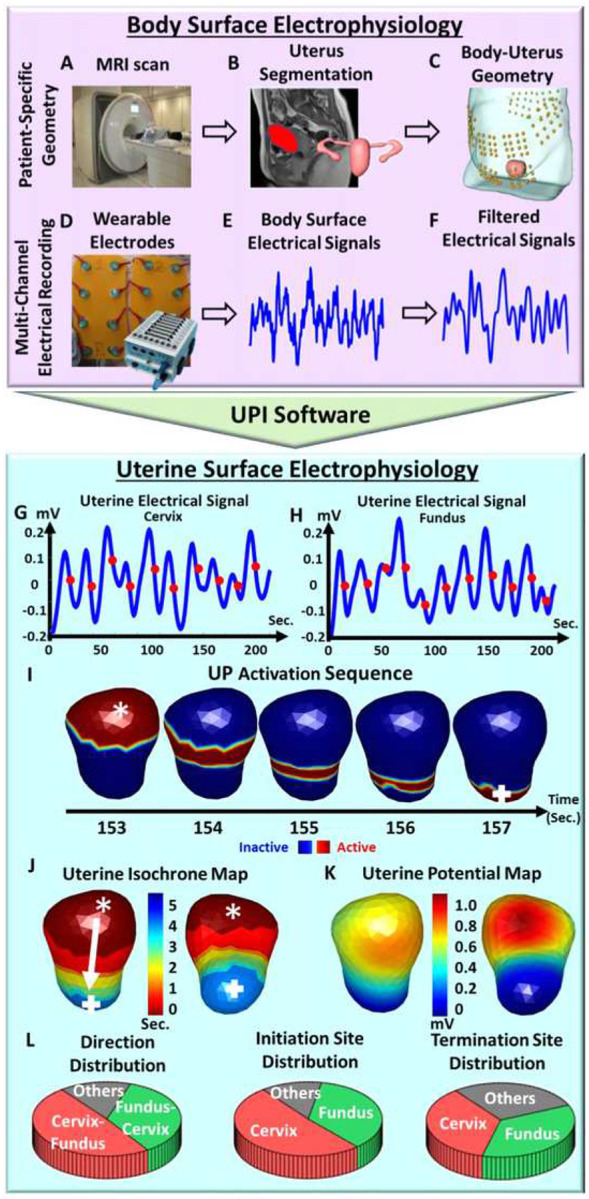
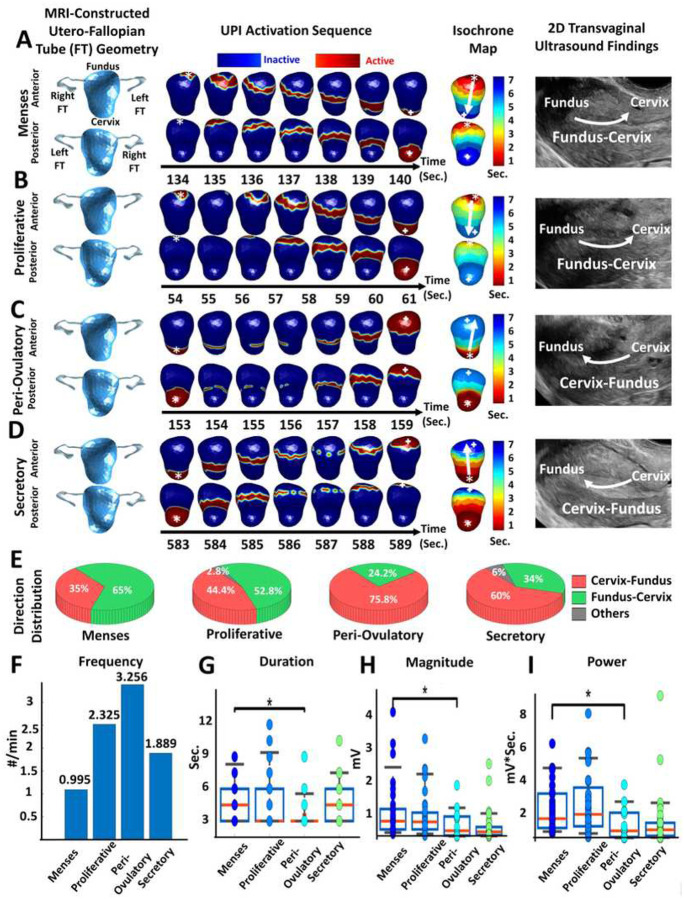
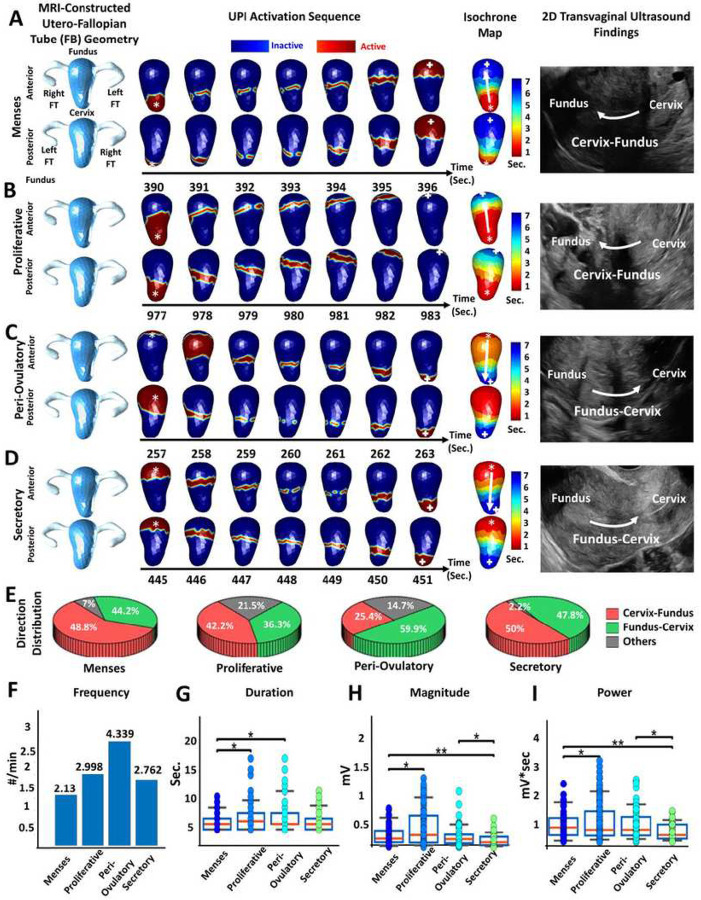
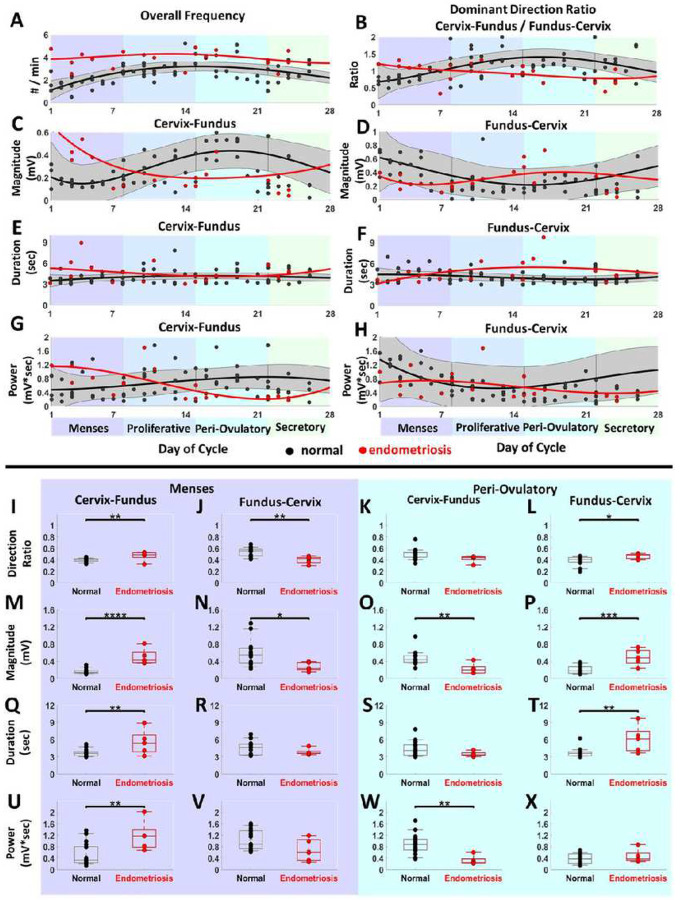
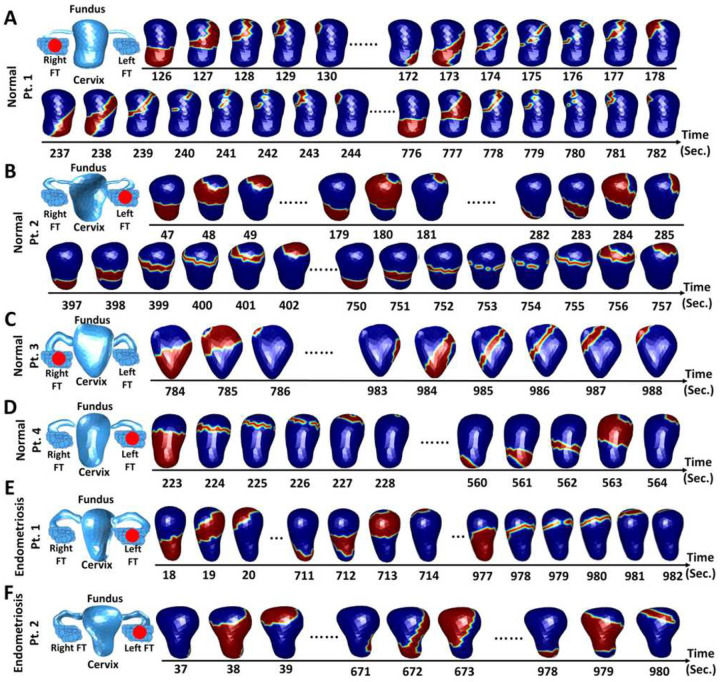
Throughout the menstrual cycle, spontaneous mild contractions in the inner layer of the uterine smooth muscle cause uterine peristalsis, which plays a critical role in normal menstruation and fertility. Disruptions in peristalsis patterns may occur in women experiencing subfertility, abnormal uterine bleeding, ovulatory dysfunction, endometriosis, and other disorders. However, current tools to measure uterine peristalsis in humans have limitations that hamper their research or clinical utilities. Here, we describe an electrophysiological imaging system to noninvasively quantify the four-dimensional (4D) electrical activation pattern during human uterine peristalsis with high spatial and temporal resolution and coverage. We longitudinally imaged 4968 uterine peristalses in 17 participants with normal gynecologic anatomy and physiology over 34 hours and 679 peristalses in 5 participants with endometriosis over 12.5 hours throughout the menstrual cycle. Our data provide quantitative evidence that uterine peristalsis changes in frequency, direction, duration, magnitude, and power throughout the menstrual cycle and is disrupted in endometriosis patients. Moreover, our data suggest that disrupted uterine peristalsis contributes to excess retrograde menstruation and infertility in patients with endometriosis and potentially contributes to infertility in this cohort.
Conflict of interest statement
Competing interests: Y.W. is a scientific consultant for Medtronic, EP solution, and has NIH research funding.
Figures
References
-
- de Vries K., Lyons E. A., Ballard G., Levi C. S. & Lindsay D. J. Contractions of the inner third of the myometrium. Am. J. Obstet. Gynecol. 162, 679–682 (1990). - PubMed
-
- Lyons E. A. et al. Characterization of subendometrial myometrial contractions throughout the menstrual cycle in normal fertile women. Fertil. Steril. 55, 771–774 (1991). - PubMed
-
- Bulletti C. et al. Uterine contractility during the menstrual cycle. Hum. Reprod. 15, 81–89 (2000). - PubMed
-
- Kunz G. & Leyendecker G. Uterine peristaltic activity during the menstrual cycle: characterization, regulation, function and dysfunction. Reprod. Biomed. Online 4 Suppl 3, 5–9 (2002). - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
