

This is a preprint.
Evaluating targeted COVID-19 vaccination strategies with agent-based modeling
- PMID: 36945423
- PMCID: PMC10029084
- DOI: 10.1101/2023.03.09.23285319
Evaluating targeted COVID-19 vaccination strategies with agent-based modeling
Update in
-
Evaluating targeted COVID-19 vaccination strategies with agent-based modeling.PLoS Comput Biol. 2024 May 31;20(5):e1012128. doi: 10.1371/journal.pcbi.1012128. eCollection 2024 May. PLoS Comput Biol. 2024. PMID: 38820570 Free PMC article.
Abstract
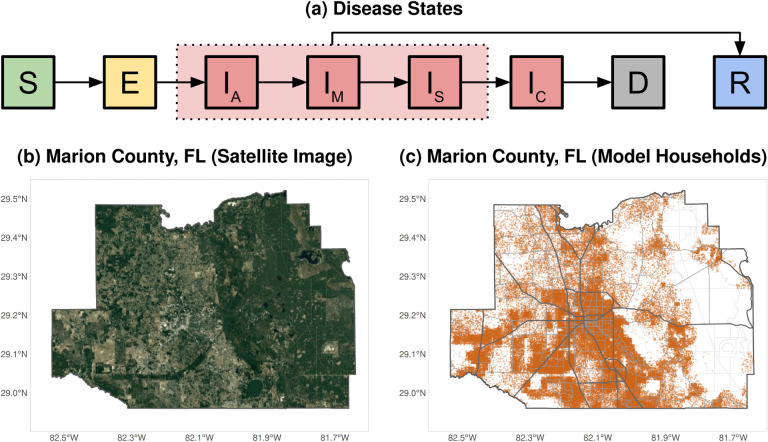
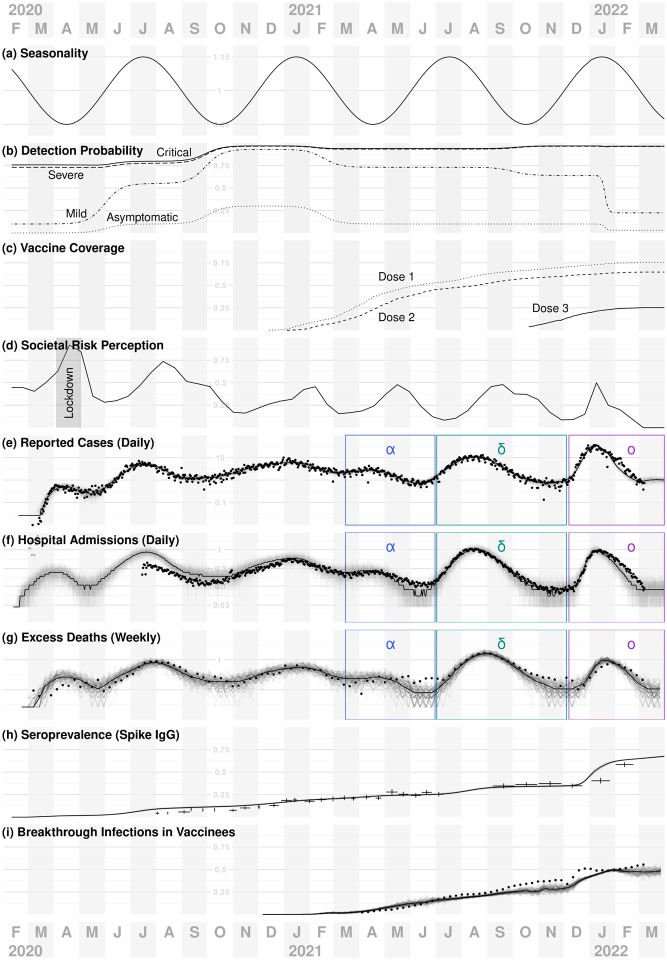
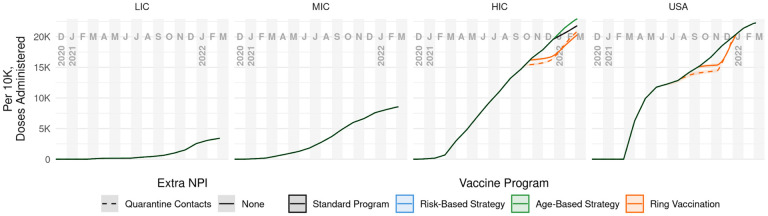
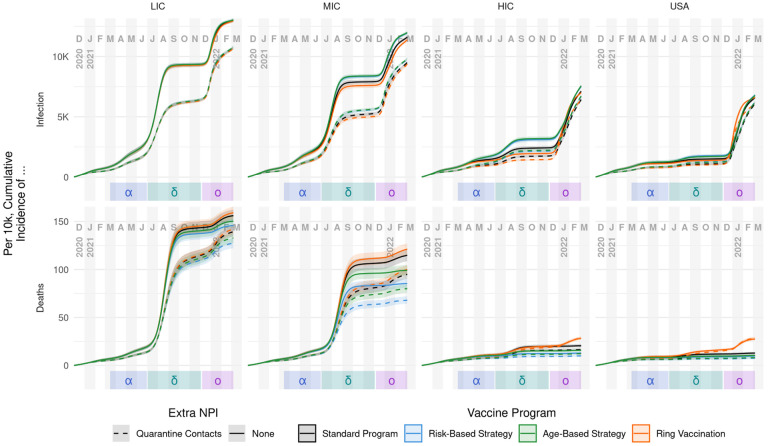
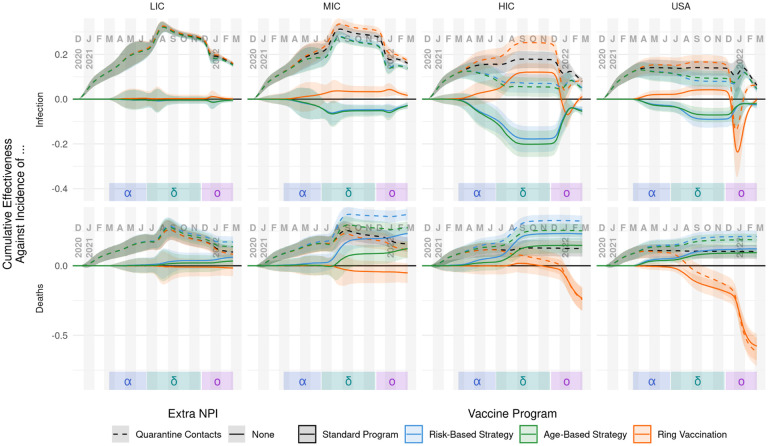
We evaluate approaches to vaccine distribution using an agent-based model of human activity and COVID-19 transmission calibrated to detailed trends in cases, hospitalizations, deaths, seroprevalence, and vaccine breakthrough infections in Florida, USA. We compare the incremental effectiveness for four different distribution strategies at four different levels of vaccine availability, reflecting different income settings' historical COVID-19 vaccine distribution. Our analysis indicates that the best strategy to reduce severe outcomes is to actively target high disease-risk individuals. This was true in every scenario, although the advantage was greatest for the middle-income-country availability assumptions, and relatively modest compared to a simple mass vaccination approach for rapid, high levels of vaccine availability. Ring vaccination, while generally the most effective strategy for reducing infections, ultimately proved least effective at preventing deaths. We also consider using age group as a practical, surrogate measure for actual disease-risk targeting; this approach still outperforms both simple mass distribution and ring vaccination. We also find that the magnitude of strategy effectiveness depends on when assessment occurs (e.g., after delta vs. after omicron variants). However, these differences in absolute benefit for the strategies do not change the ranking of their performance at preventing severe outcomes across vaccine availability assumptions.
Keywords: Agent-based Model; COVID-19; Florida; LMIC; Ring Vaccination; Vaccination.
Figures

References
-
- Assistant Secretary for Public Affairs (ASPA), COVID-19 Vaccines (2020).
-
- Ebola ça suffit ring vaccination trial consortium, British Medical Journal 351 (2015).
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources