

A pooled analysis of the risk prediction models for mortality in acute exacerbation of chronic obstructive pulmonary disease
- PMID: 36945821
- PMCID: PMC10435958
- DOI: 10.1111/crj.13606
A pooled analysis of the risk prediction models for mortality in acute exacerbation of chronic obstructive pulmonary disease
Abstract
Objective: The prognosis for acute exacerbation of chronic obstructive pulmonary disease (AECOPD) is not optimistic, and severe AECOPD leads to an increased risk of mortality. Prediction models help distinguish between high- and low-risk groups. At present, many prediction models have been established and validated, which need to be systematically reviewed to screen out more suitable models that can be used in the clinic and provide evidence for future research.
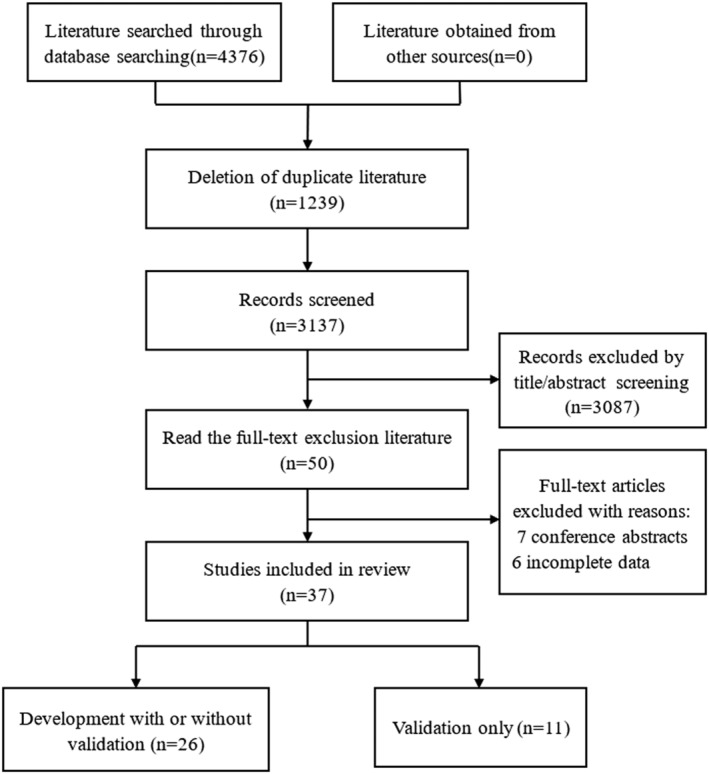
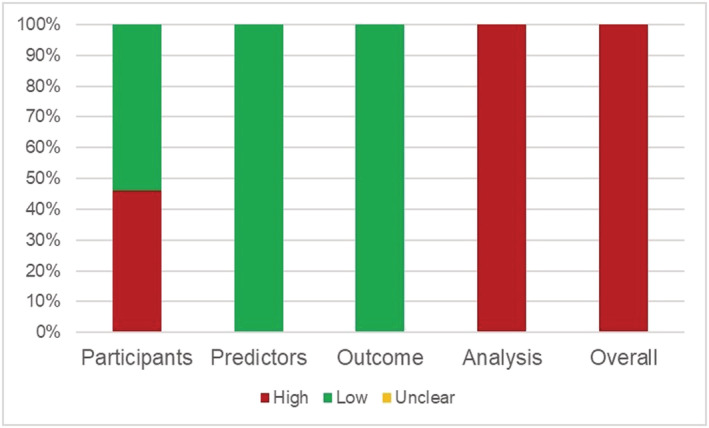
Methods: We searched PubMed, EMBASE, Cochrane Library and Web of Science databases for studies on risk models for AECOPD mortality from their inception to 10 April 2022. The risk of bias was assessed using the prediction model risk of bias assessment tool (PROBAST). Stata software (version 16) was used to synthesize the C-statistics for each model.
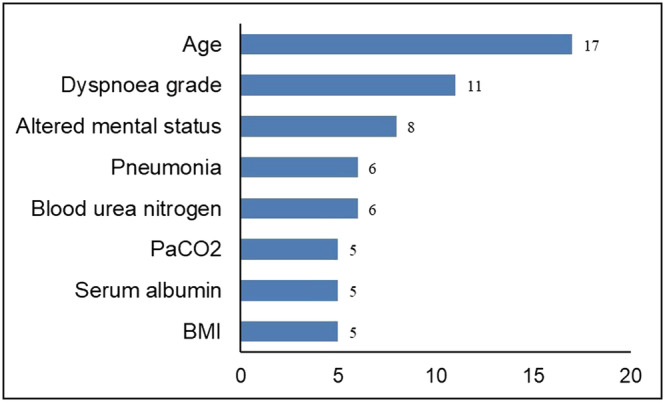
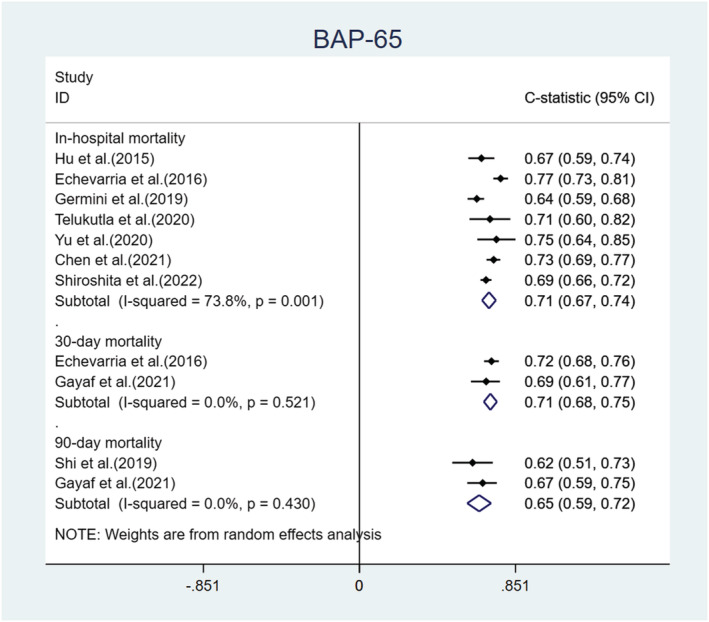
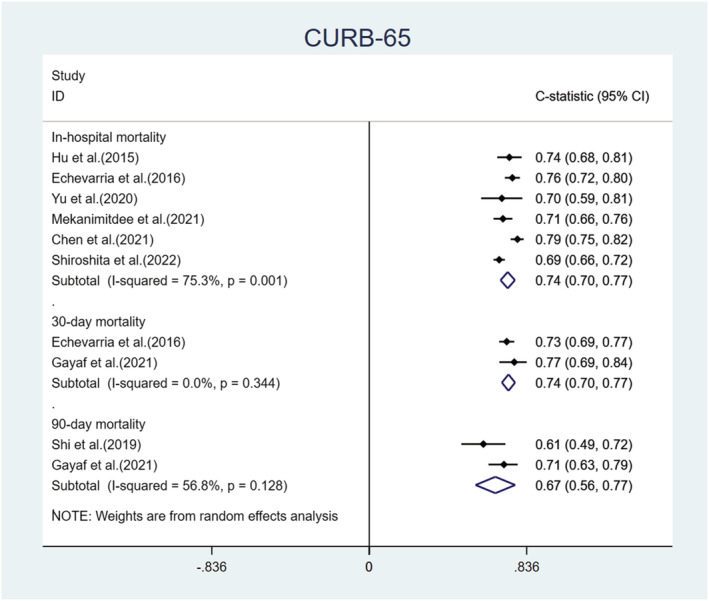
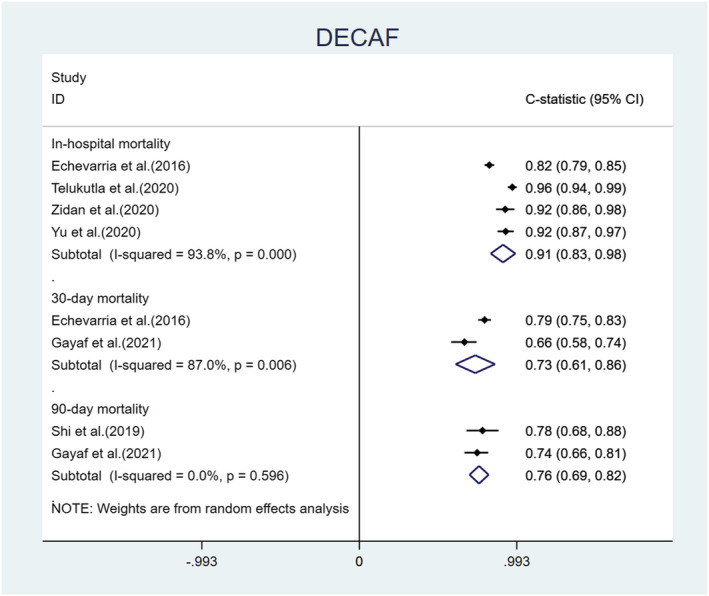
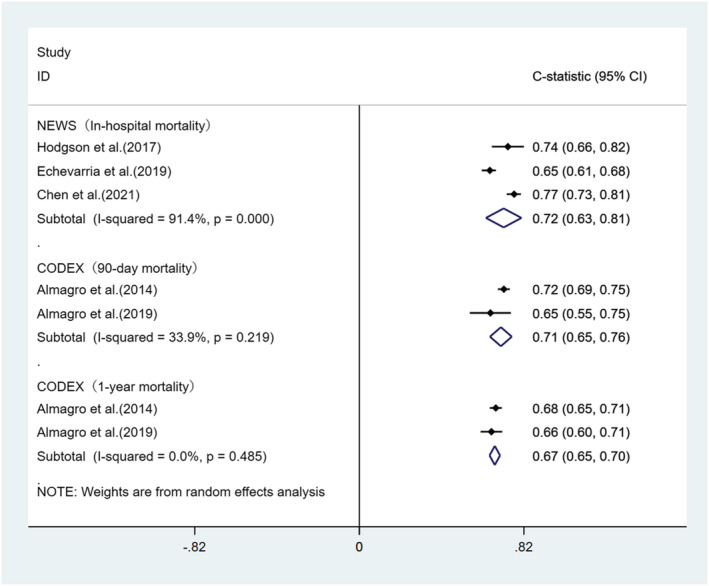
Results: A total of 37 studies were included. The development of risk prediction models for mortality in patients with AECOPD was described in 26 articles, in which the most common predictors were age (n = 17), dyspnea grade (n = 11), altered mental status (n = 8), pneumonia (n = 6) and blood urea nitrogen (BUN, n = 6). The remaining 11 articles only externally validated existing models. All 37 studies were evaluated at a high risk of bias using PROBAST. We performed a meta-analysis of five models included in 15 studies. DECAF (dyspnoea, eosinopenia, consolidation, acidemia and atrial fibrillation) performed well in predicting in-hospital death [C-statistic = 0.91, 95% confidence interval (CI): 0.83, 0.98] and 90-day death [C-statistic = 0.76, 95% CI: 0.69, 0.82] and CURB-65 (confusion, urea, respiratory rate, blood pressure and age) performed well in predicting 30-day death [C-statistic = 0.74, 95% CI: 0.70, 0.77].
Conclusions: This study provides information on the characteristics, performance and risk of bias of a risk model for AECOPD mortality. This pooled analysis of the present study suggests that the DECAF performs well in predicting in-hospital and 90-day deaths. Yet, external validation in different populations is still needed to prove this performance.
Keywords: AECOPD; mortality; pooled analysis; prediction models.
© 2023 The Authors. The Clinical Respiratory Journal published by John Wiley & Sons Ltd.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Global Initiative for Chronic Obstructive Lung Disease . (updated 2022). Global strategy for the diagnosis, management and prevention of chronic obstructive pulmonary disease. Accessed April 23, 2022. https://goldcopd.org/2022-gold-reports-2/
Publication types
MeSH terms
Grants and funding
- 2018YFC1704806/National Key R&D Program
- 212102311128/Henan Science and Technology Research Project
- 212300410056/Natural Science Foundation of Henan Youth Fund
- STG-ZYX01-202102/Henan Province Priority and Advantage Discipline Construction Engineering Projects-Traditional Chinese Medicine
- LHGJ20220586/Henan Medical Science and Technology Research Program
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
