

Metastatic Pheochromocytoma and Paraganglioma: Somatostatin Receptor 2 Expression, Genetics, and Therapeutic Responses
- PMID: 36946182
- PMCID: PMC10505550
- DOI: 10.1210/clinem/dgad166
Metastatic Pheochromocytoma and Paraganglioma: Somatostatin Receptor 2 Expression, Genetics, and Therapeutic Responses
Abstract
Context: Pheochromocytomas and paragangliomas (PPGLs) with pathogenic mutations in the succinate dehydrogenase subunit B (SDHB) are associated with a high metastatic risk. Somatostatin receptor 2 (SSTR2)-dependent imaging is the most sensitive imaging modality for SDHB-related PPGLs, suggesting that SSTR2 expression is a significant cell surface therapeutic biomarker of such tumors.
Objective: Exploration of the relationship between SSTR2 immunoreactivity and SDHB immunoreactivity, mutational status, and clinical behavior of PPGLs. Evaluation of SSTR-based therapies in metastatic PPGLs.
Methods: Retrospective analysis of a multicenter cohort of PPGLs at 6 specialized Endocrine Tumor Centers in Germany, The Netherlands, and Switzerland. Patients with PPGLs participating in the ENSAT registry were included. Clinical data were extracted from medical records, and immunohistochemistry (IHC) for SDHB and SSTR2 was performed in patients with available tumor tissue. Immunoreactivity of SSTR2 was investigated using Volante scores. The main outcome measure was the association of SSTR2 IHC positivity with genetic and clinical-pathological features of PPGLs.
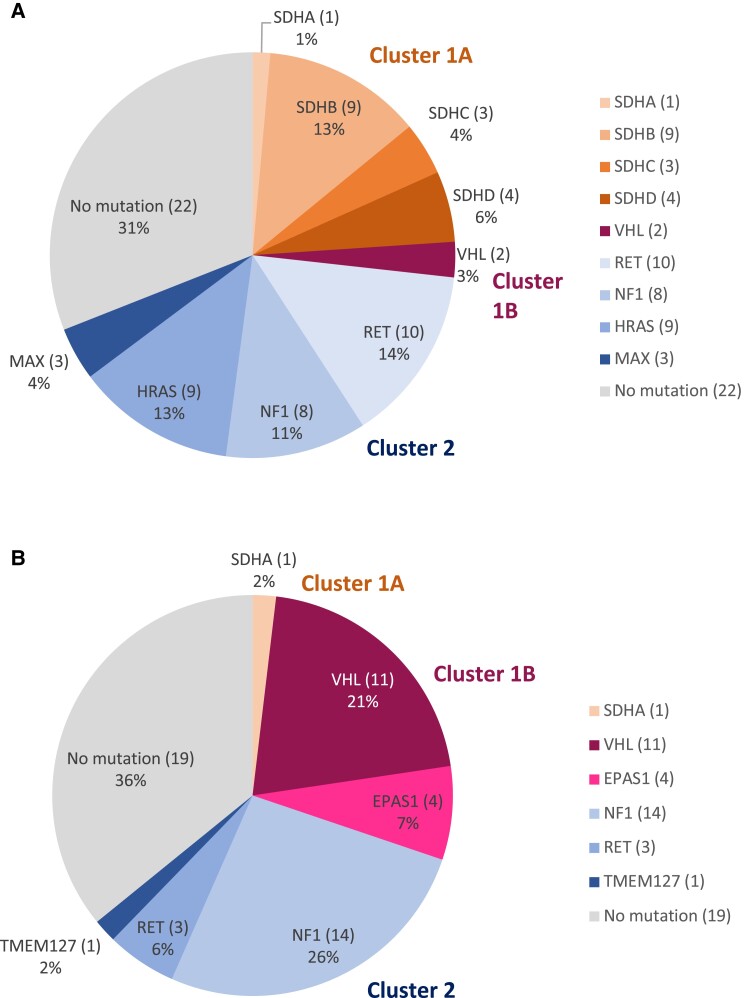
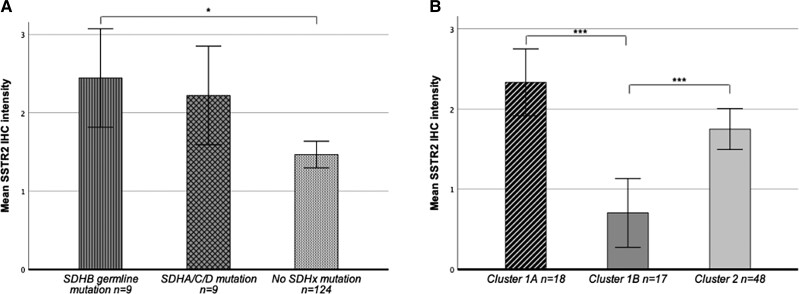
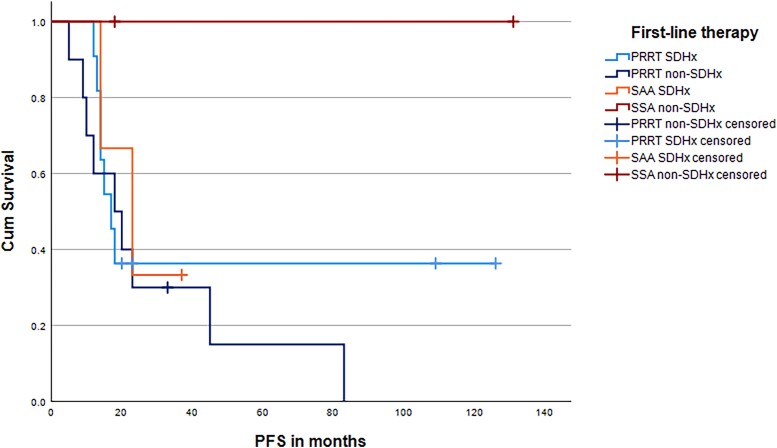
Results: Of 202 patients with PPGLs, 50% were SSTR2 positive. SSTR2 positivity was significantly associated with SDHB- and SDHx-related PPGLs, with the strongest SSTR2 staining intensity in SDHB-related PPGLs (P = .01). Moreover, SSTR2 expression was significantly associated with metastatic disease independent of SDHB/SDHx mutation status (P < .001). In metastatic PPGLs, the disease control rate with first-line SSTR-based radionuclide therapy was 67% (n = 22, n = 11 SDHx), and with first-line "cold" somatostatin analogs 100% (n = 6, n = 3 SDHx).
Conclusion: SSTR2 expression was independently associated with SDHB/SDHx mutations and metastatic disease. We confirm a high disease control rate of somatostatin receptor-based therapies in metastatic PPGLs.
Keywords: SDHB mutation; SDHx mutation; PRRT; metastatic pheochromocytoma/paraganglioma; somatostatin receptor 2; somatostatin receptor–based therapies.
© The Author(s) 2023. Published by Oxford University Press on behalf of the Endocrine Society.
Figures
References
-
- Dahia PLM. Pheochromocytoma and paraganglioma pathogenesis: learning from genetic heterogeneity. Nat Rev Cancer. 2014;14(2):108‐119. - PubMed
-
- Hescot S, Curras-Freixes M, Deutschbein T, et al. Prognosis of malignant pheochromocytoma and paraganglioma (MAPP-prono study): a European network for the study of adrenal tumors retrospective study. J Clin Endocrinol Metab. 2019;104(6):2367‐2374. - PubMed
-
- Lenders JWM, Kerstens MN, Amar L, et al. Genetics, diagnosis, management and future directions of research of phaeochromocytoma and paraganglioma: a position statement and consensus of the working group on endocrine hypertension of the European Society of hypertension. J Hypertens. 2020;38(8):1443‐1456. - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
