

Effects of Standard-Dose Prophylactic, High-Dose Prophylactic, and Therapeutic Anticoagulation in Patients With Hypoxemic COVID-19 Pneumonia: The ANTICOVID Randomized Clinical Trial
- PMID: 36946232
- PMCID: PMC10034664
- DOI: 10.1001/jamainternmed.2023.0456
Effects of Standard-Dose Prophylactic, High-Dose Prophylactic, and Therapeutic Anticoagulation in Patients With Hypoxemic COVID-19 Pneumonia: The ANTICOVID Randomized Clinical Trial
Abstract
Importance: Given the high risk of thrombosis and anticoagulation-related bleeding in patients with hypoxemic COVID-19 pneumonia, identifying the lowest effective dose of anticoagulation therapy for these patients is imperative.
Objectives: To determine whether therapeutic anticoagulation (TA) or high-dose prophylactic anticoagulation (HD-PA) decreases mortality and/or disease duration compared with standard-dose prophylactic anticoagulation (SD-PA), and whether TA outperforms HD-PA; and to compare the net clinical outcomes among the 3 strategies.
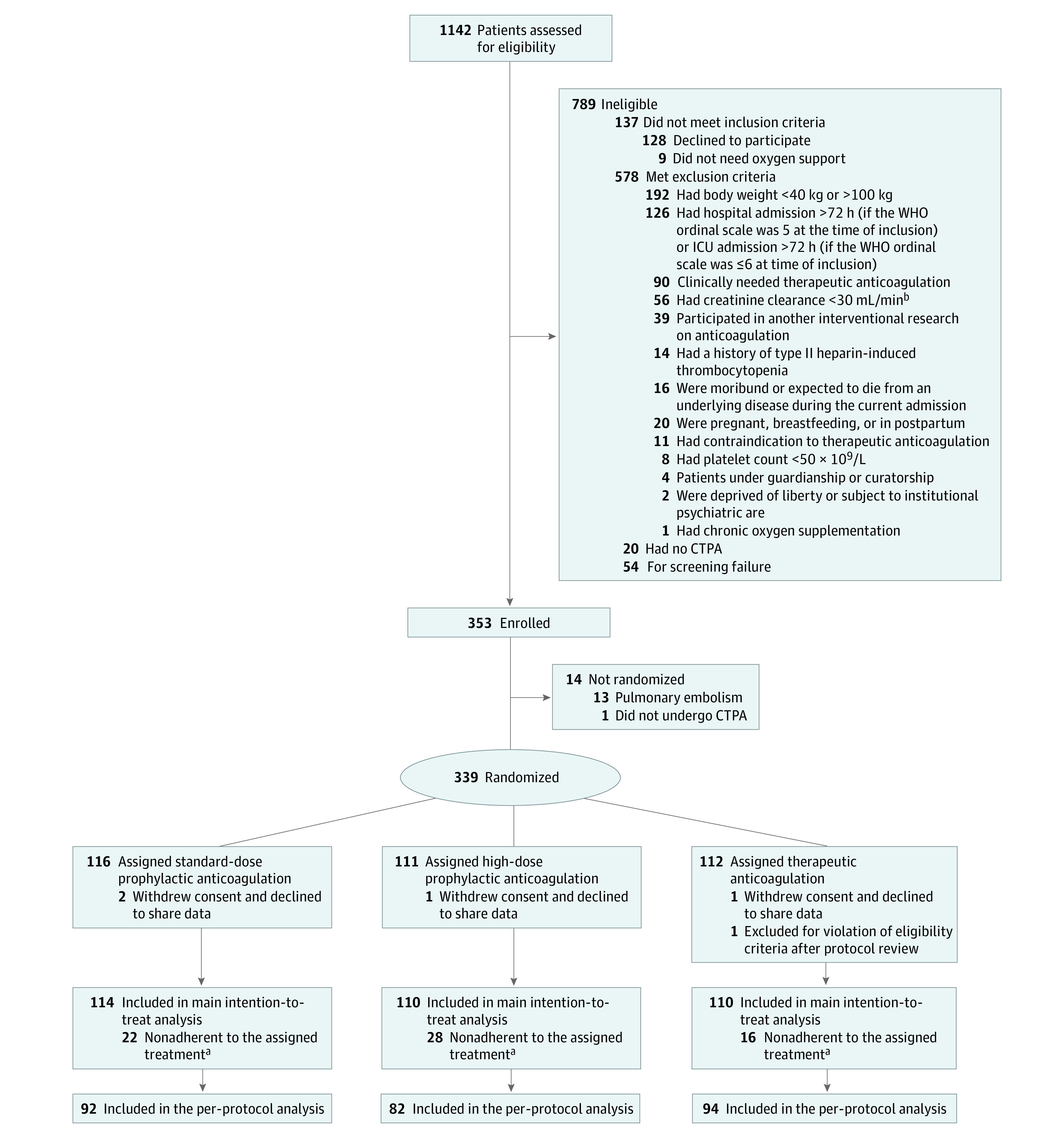
Design, settings, and participants: The ANTICOVID randomized clinical open-label trial included patients with hypoxemic COVID-19 pneumonia requiring supplemental oxygen and having no initial thrombosis on chest computer tomography with pulmonary angiogram at 23 health centers in France from April 14 to December 13, 2021. Of 339 patients randomized, 334 were included in the primary analysis-114 patients in the SD-PA group, 110 in the HD-PA, and 110 in the TA. At randomization, 90% of the patients were in the intensive care unit. Data analyses were performed from April 13, 2022, to January 3, 2023.
Interventions: Patients were randomly assigned (1:1:1) to receive either SD-PA, HD-PA, or TA with low-molecular-weight or unfractionated heparin for 14 days.
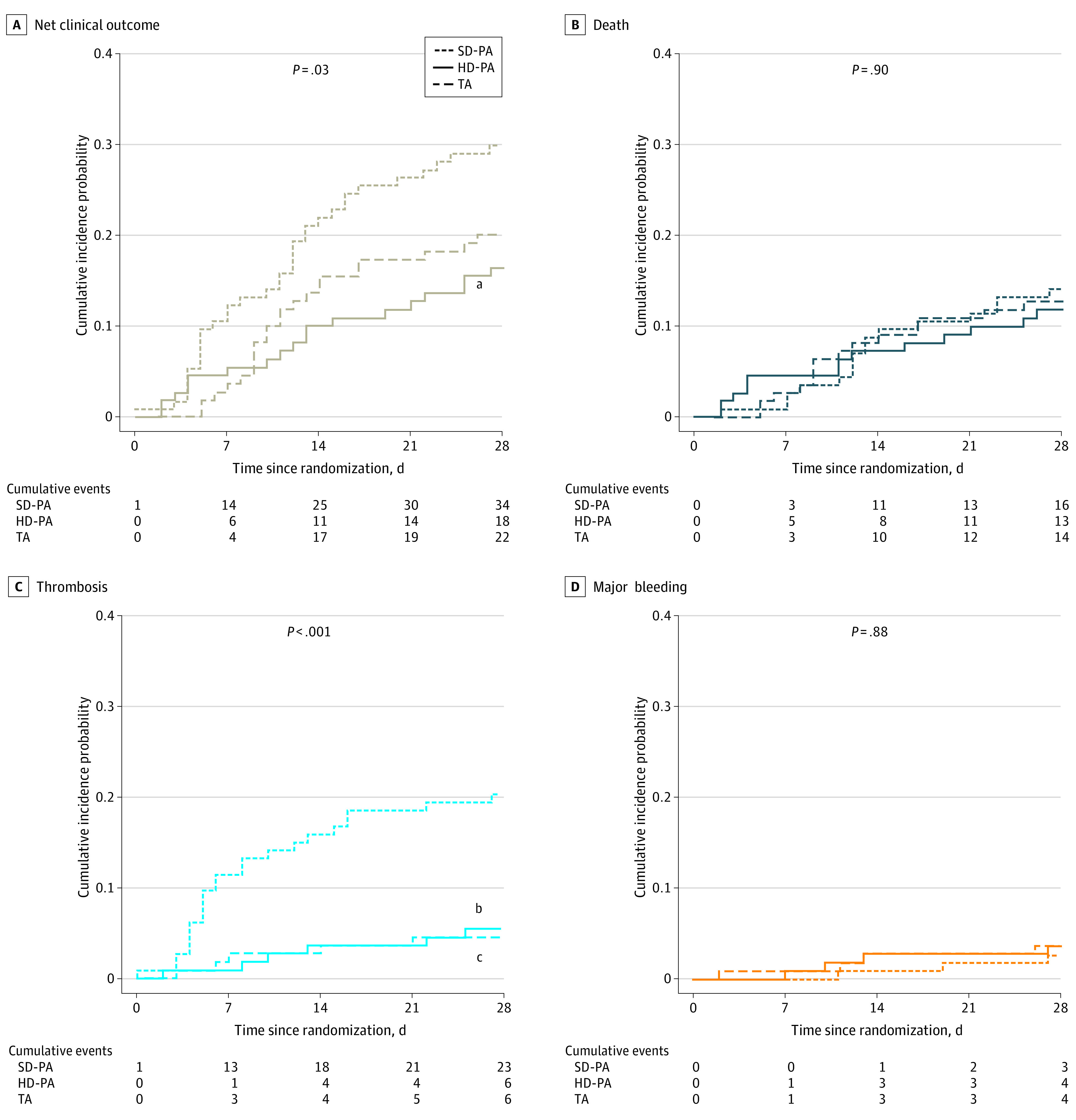
Main outcomes and measures: A hierarchical criterion of all-cause mortality followed by time to clinical improvement at day 28. Main secondary outcome was net clinical outcome at day 28 (composite of thrombosis, major bleeding, and all-cause death).
Results: Among the study population of 334 individuals (mean [SD] age, 58.3 [13.0] years; 226 [67.7%] men and 108 [32.3%] women), use of HD-PA and SD-PA had similar probabilities of favorable outcome (47.3% [95% CI, 39.9% to 54.8%] vs 52.7% [95% CI, 45.2% to 60.1%]; P = .48), as did TA compared with SD-PA (50.9% [95% CI, 43.4% to 58.3%] vs 49.1% [95% CI, 41.7% to 56.6%]; P = .82) and TA compared with HD-PA (53.5% [95% CI 45.8% to 60.9%] vs 46.5% [95% CI, 39.1% to 54.2%]; P = .37). Net clinical outcome was met in 29.8% of patients receiving SD-PA (20.2% thrombosis, 2.6% bleeding, 14.0% death), 16.4% receiving HD-PA (5.5% thrombosis, 3.6% bleeding, 11.8% death), and 20.0% receiving TA (5.5% thrombosis, 3.6% bleeding, 12.7% death). Moreover, HD-PA and TA use significantly reduced thrombosis compared with SD-PA (absolute difference, -14.7 [95% CI -6.2 to -23.2] and -14.7 [95% CI -6.2 to -23.2], respectively). Use of HD-PA significantly reduced net clinical outcome compared with SD-PA (absolute difference, -13.5; 95% CI -2.6 to -24.3).
Conclusions and relevance: This randomized clinical trial found that compared with SD-PA, neither HD-PA nor TA use improved the primary hierarchical outcome of all-cause mortality or time to clinical improvement in patients with hypoxemic COVID-19 pneumonia; however, HD-PA resulted in significantly better net clinical outcome by decreasing the risk of de novo thrombosis.
Trial registration: ClinicalTrials.gov Identifier: NCT04808882.
Conflict of interest statement
Figures
Comment in
-
Anticoagulation in Patients With COVID-19 Pneumonia-What Is the Optimal Intensity?JAMA Intern Med. 2023 Jun 1;183(6):532-533. doi: 10.1001/jamainternmed.2023.0625. JAMA Intern Med. 2023. PMID: 36946227 No abstract available.
References
-
- Bikdeli B, Madhavan MV, Jimenez D, et al. ; Global COVID-19 Thrombosis Collaborative Group . COVID-19 and thrombotic or thromboembolic disease: implications for prevention, antithrombotic therapy, and follow-up: JACC state-of-the-art review. J Am Coll Cardiol. 2020;75(23):2950-2973. doi: 10.1016/j.jacc.2020.04.031 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
