

Combined radiation injury and its impacts on radiation countermeasures and biodosimetry
- PMID: 36947602
- PMCID: PMC10947598
- DOI: 10.1080/09553002.2023.2188933
Combined radiation injury and its impacts on radiation countermeasures and biodosimetry
Abstract
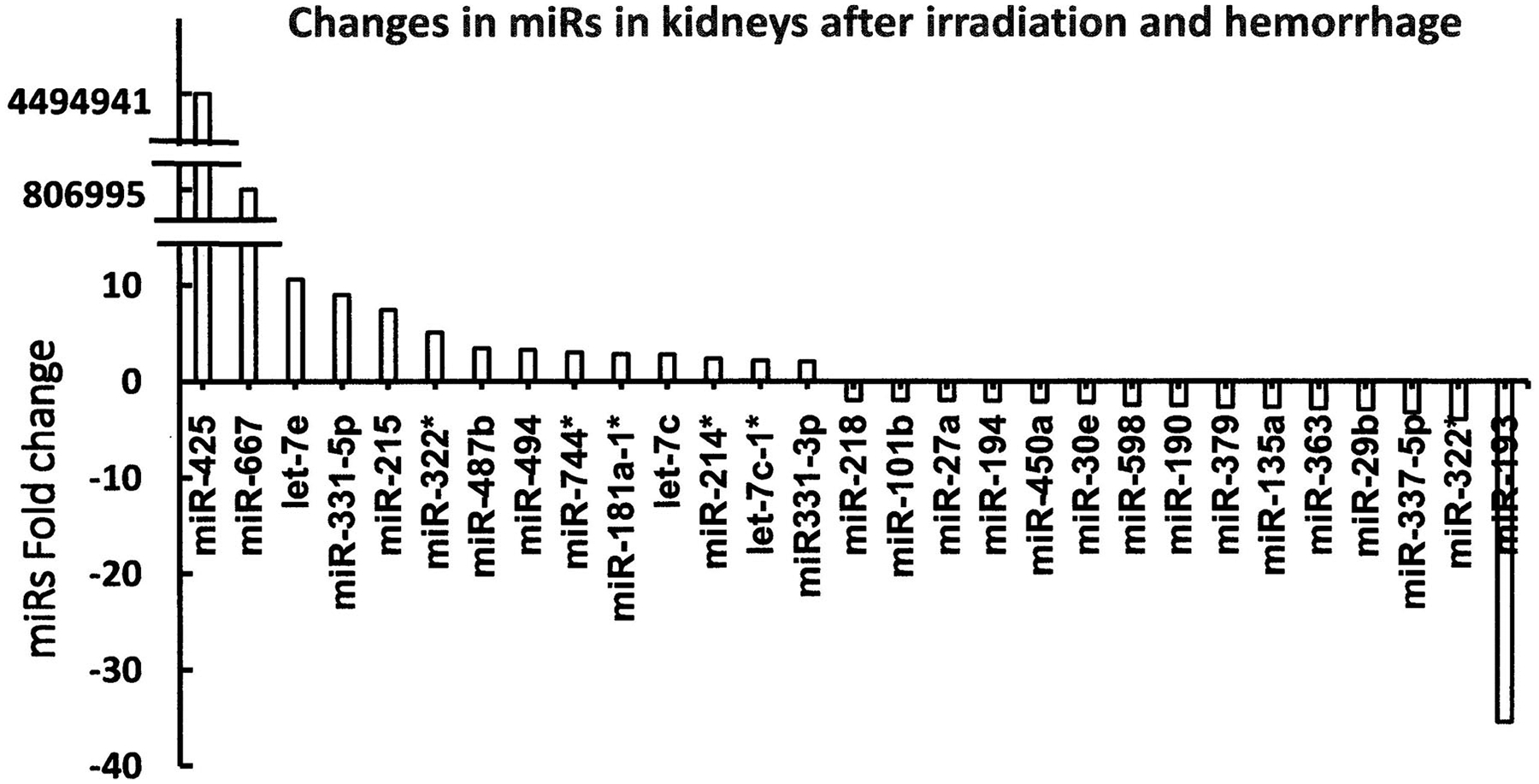
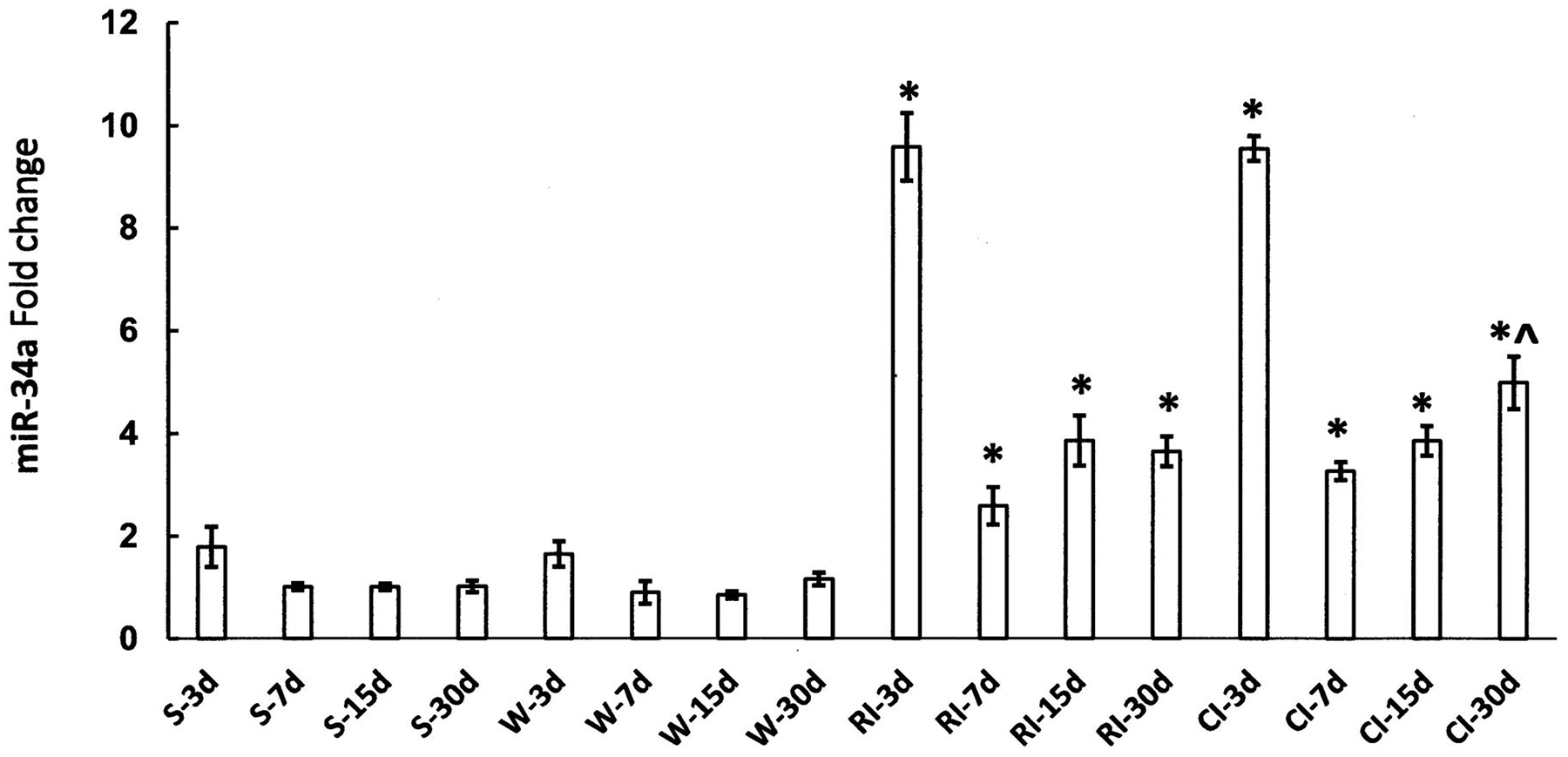
Purpose: Preparedness for medical responses to major radiation accidents and the increasing threat of nuclear warfare worldwide necessitates an understanding of the complexity of combined radiation injury (CI) and identifying drugs to treat CI is inevitably critical. The vital sign and survival after CI were presented. The molecular mechanisms, such as microRNA pathways, NF-κB-iNOS-IL-18 pathway, C3 production, the AKT-MAPK cross-talk, and TLR/MMP increases, underlying CI in relation to organ injury and mortality were analyzed. At present, no FDA-approved drug to protect, mitigate, or treat CI is available. The development of CI-specific medical countermeasures was reviewed. Because of the worsened acute radiation syndrome resulting from CI, diagnostic triage can be problematic. Therefore, biodosimetry and CI are bundled together with the need to establish effective triage methods with CI.
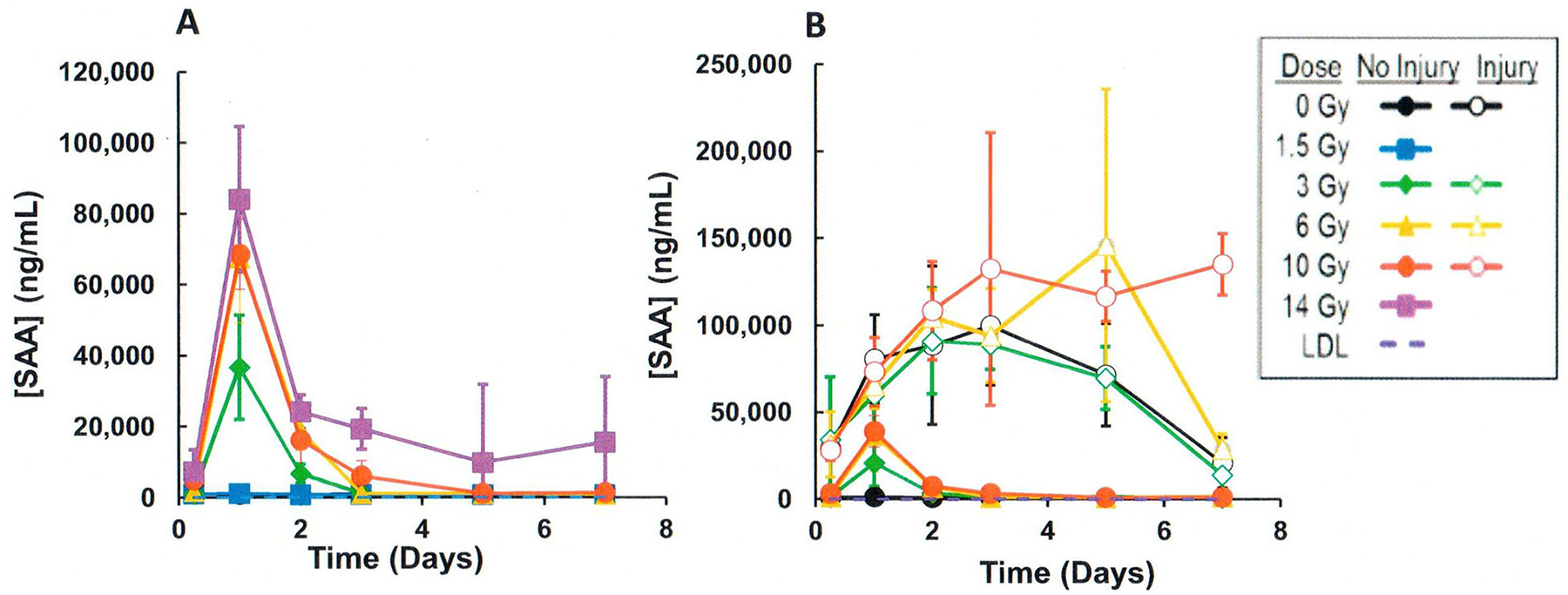
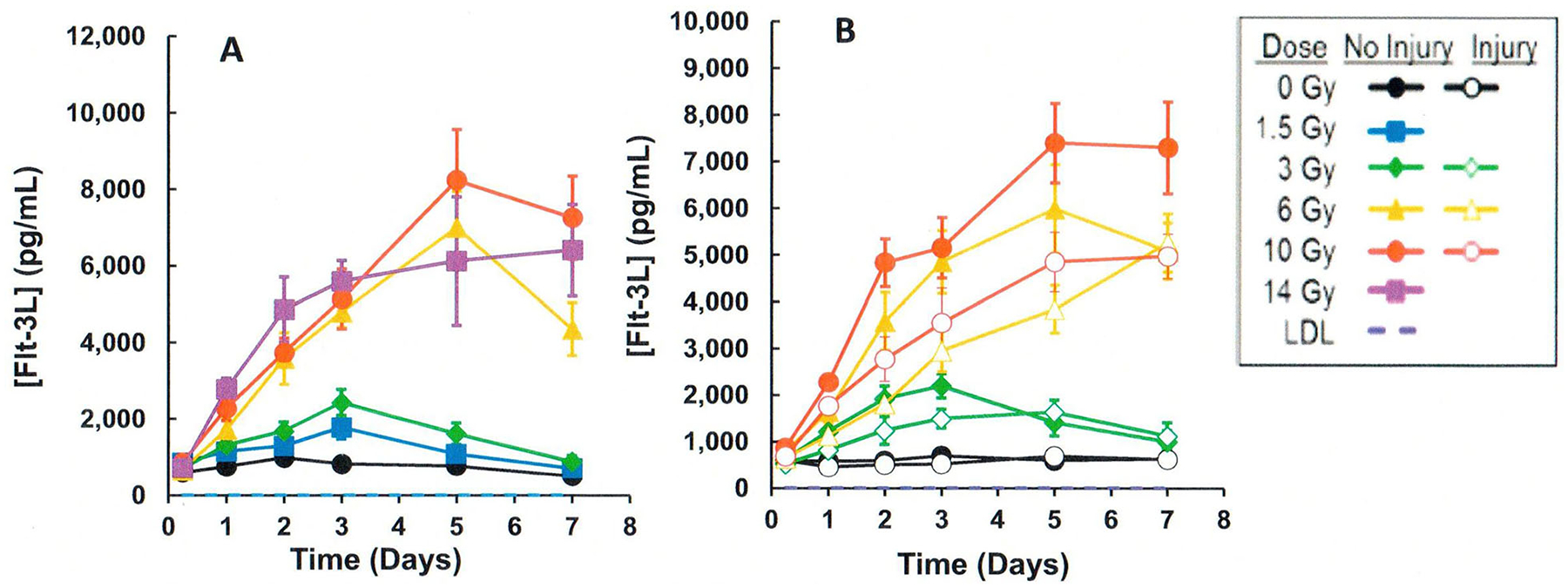
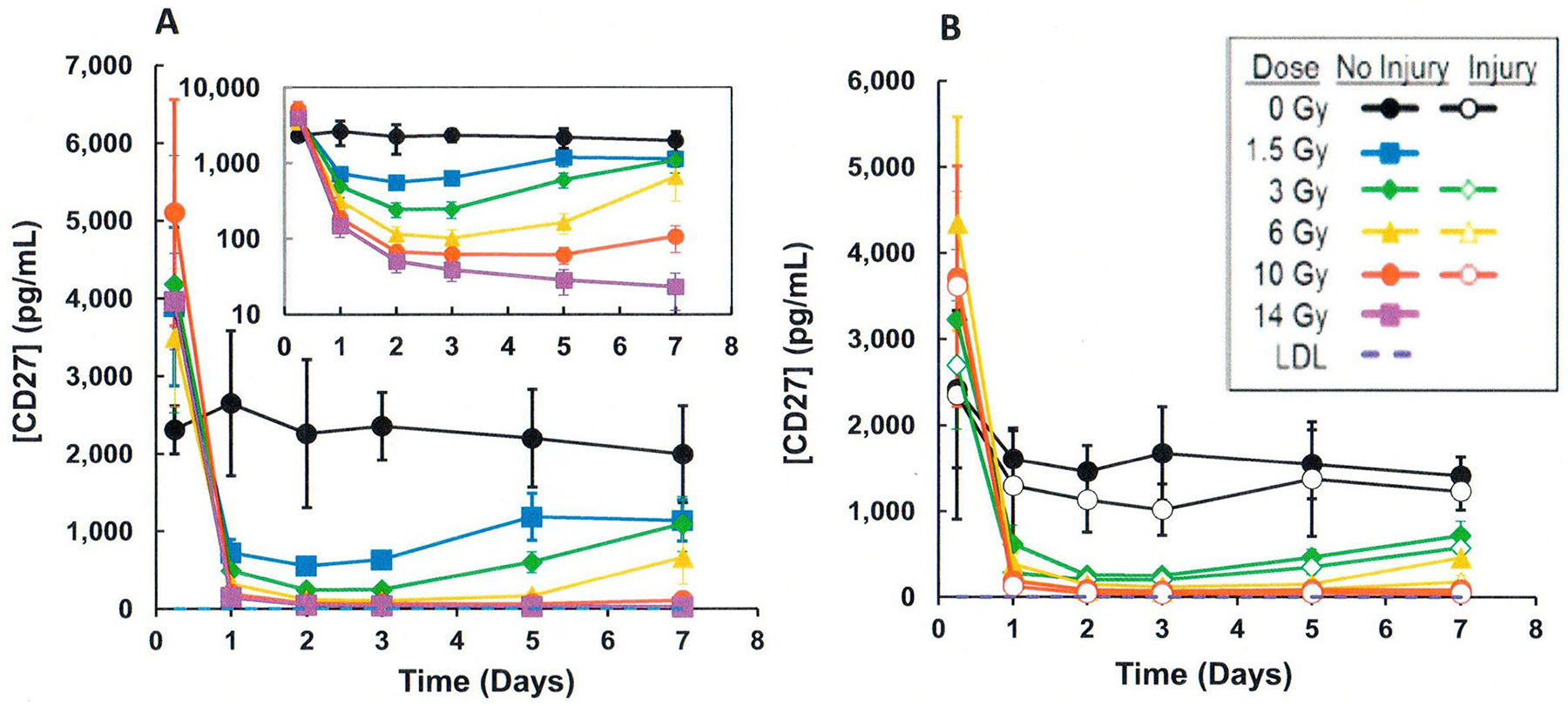
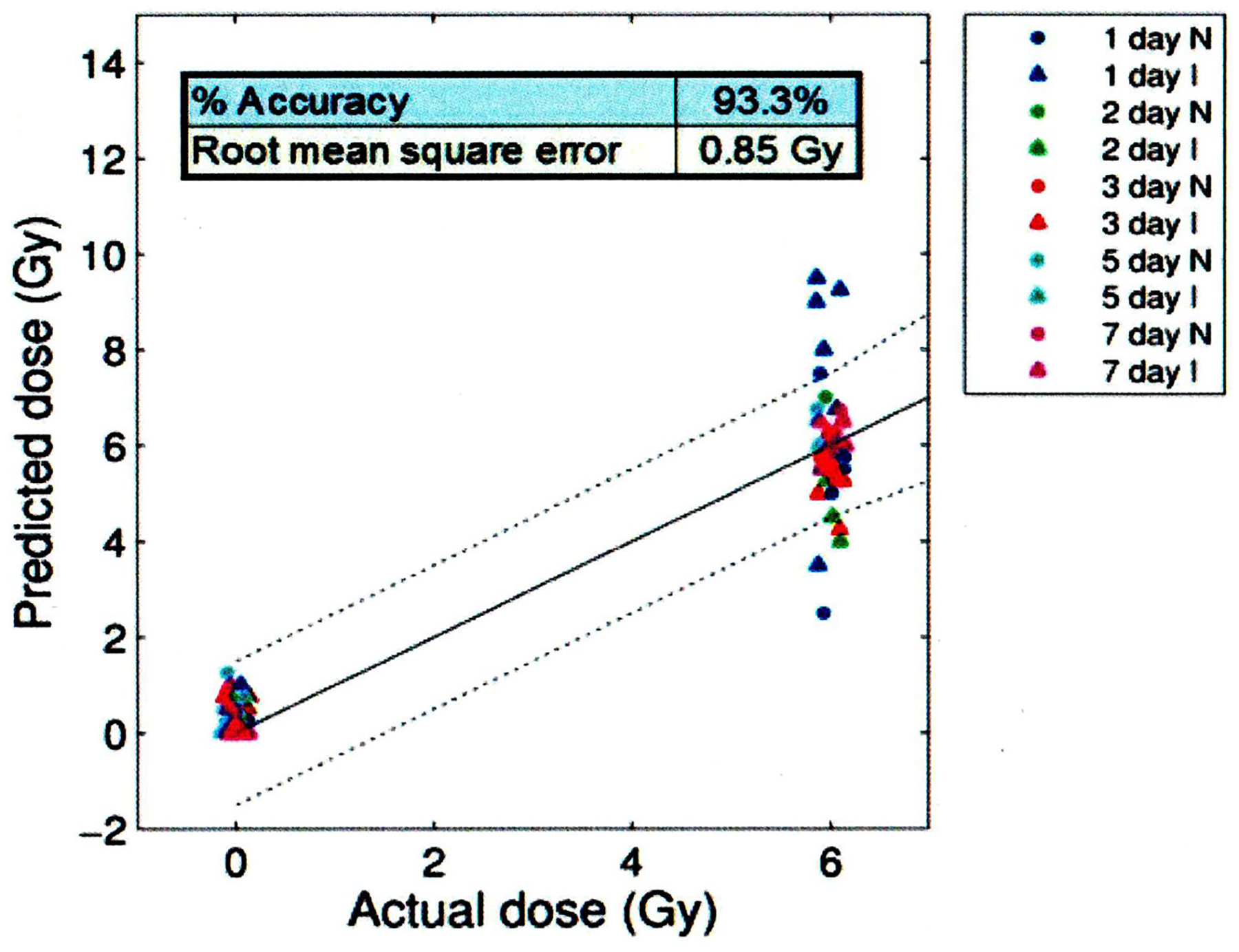
Conclusions: CI mouse model studies at AFRRI are reviewed addressing molecular responses, findings from medical countermeasures, and a proposed plasma proteomic biodosimetry approach based on a panel of radiation-responsive biomarkers (i.e., CD27, Flt-3L, GM-CSF, CD45, IL-12, TPO) negligibly influenced by wounding in an algorithm used for dose predictions is described.
Keywords: Combined radiation injury; acute radiation syndrome; biodosimetry; mechanisms; medical countermeasures; wounding.
Conflict of interest statement
Disclosure statement
The authors report no financial conflicts of interest. The manuscript was cleared for publication by the Armed Forces Radiobiology Research Institute, The Uniformed Services of the Health Sciences. The views, opinions, and findings contained in this report are those of the authors and do not reflect official policy or positions of the Armed Forces Radiobiology Research Institute, the Uniformed Services University of the Health Sciences, the Department of Defense, or the United States government.
Figures
References
-
- Amgen Inc. 2015a. NEULASTA® (pegfilgrastim) injection, for subcutaneous use.
-
- Amgen Inc. 2015b. Neupogen (filgrastim) injection for subcutaneous or intravenous use.
-
- Amgen Inc. 2021. NPLATE® (romiplostim) for injection, for subcutaneous use.
-
- Barabanova AV. 2006. Significance of beta-radiation skin burns in Chernobyl patients for the theory and practice of radiopathology. Vojnosanit Pregl. 63(5):477–480. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous