

Supplemental oxygen and noninvasive ventilation
- PMID: 36948502
- PMCID: PMC10032613
- DOI: 10.1183/16000617.0159-2022
Supplemental oxygen and noninvasive ventilation
Abstract
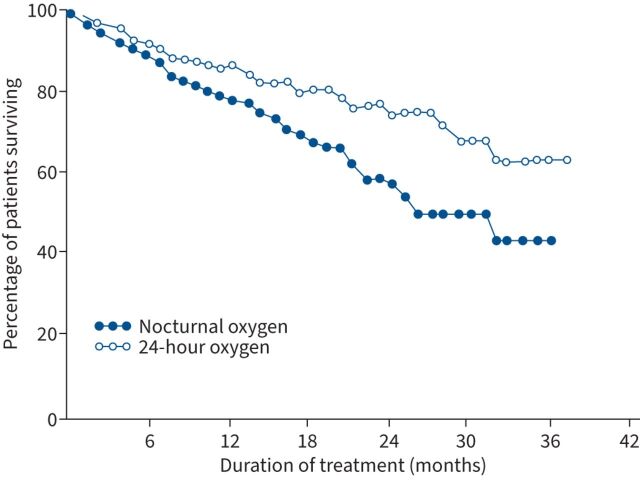
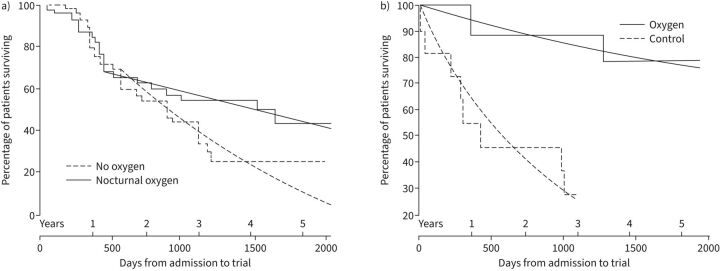
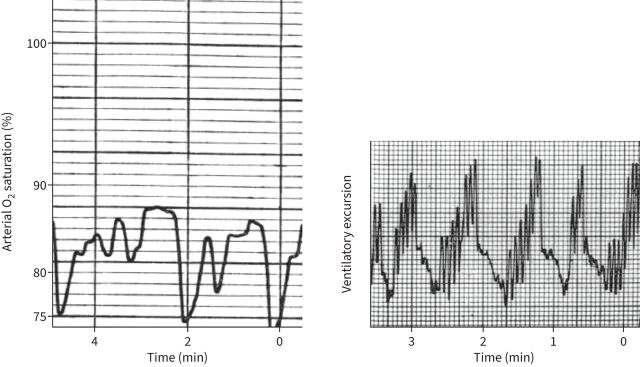
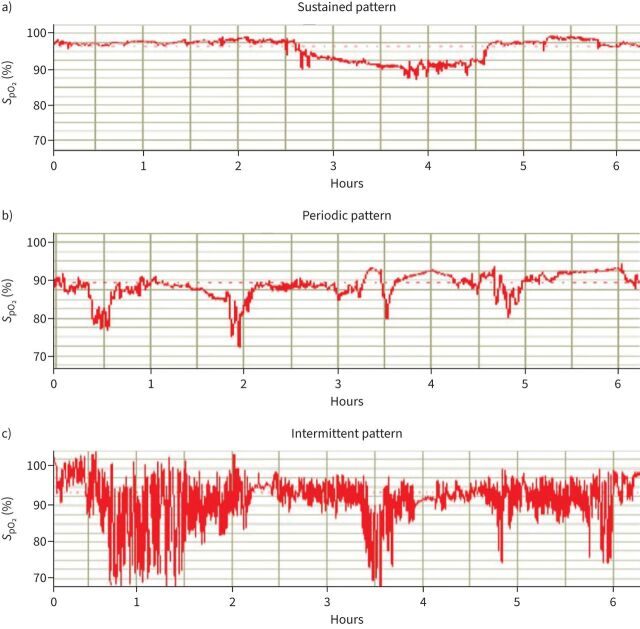
The respiratory system attempts to maintain normal levels of oxygen and carbon dioxide. However, airflow limitation, parenchymal abnormalities and dysfunction of the respiratory pump may be compromised in individuals with advanced COPD, eventually leading to respiratory failure, with reduced arterial oxygen tension (hypoxaemia) and/or increased arterial carbon dioxide tension (P aCO2 ; hypercapnia). Hypoxaemia may persist in individuals with severe COPD despite smoking cessation and optimisation of pharmacotherapy. Long-term oxygen therapy (LTOT) can improve survival in those with severe daytime hypoxaemia, whereas those with less severe hypoxaemia may only have improved exercise capacity and dyspnoea. Changes in respiratory physiology that occur during sleep further predispose to hypoxaemia, particularly in individuals with COPD. However, the major cause of hypoxaemia is hypoventilation. Noninvasive ventilation (NIV) may reduce mortality and need for intubation in individuals with COPD and acute hypercapnic respiratory failure. However, NIV may also improve survival and quality of life in individuals with stable, chronic hypercapnia and is now suggested for those with prolonged hypercapnia (e.g. P aCO2 >55 mmHg 2-6 weeks after hospital discharge) when clinically stable and after optimisation of medical therapy including LTOT if indicated. Many questions remain about the optimal mode, settings and goal of NIV therapy.
Copyright ©The authors 2023.
Conflict of interest statement
Conflict of interest: R.L. Owens has received grant NIH/NHLBI R01HL142114 paid to his institution, outside the submitted work. The remaining authors have nothing to disclose.
Figures
Comment in
-
Nonpharmacological interventions in COPD.Eur Respir Rev. 2023 Mar 22;32(167):230028. doi: 10.1183/16000617.0028-2023. Print 2023 Mar 31. Eur Respir Rev. 2023. PMID: 36948503 Free PMC article.
References
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical