

Comparative effectiveness and safety of analgesic medicines for adults with acute non-specific low back pain: systematic review and network meta-analysis
- PMID: 36948512
- PMCID: PMC10540836
- DOI: 10.1136/bmj-2022-072962
Comparative effectiveness and safety of analgesic medicines for adults with acute non-specific low back pain: systematic review and network meta-analysis
Abstract
Objective: To evaluate the comparative effectiveness and safety of analgesic medicines for acute non-specific low back pain.
Design: Systematic review and network meta-analysis.
Data sources: Medline, PubMed, Embase, CINAHL, CENTRAL, ClinicalTrials.gov, clinicialtrialsregister.eu, and World Health Organization's International Clinical Trials Registry Platform from database inception to 20 February 2022.
Eligibility criteria for study selection: Randomised controlled trials of analgesic medicines (eg, non-steroidal anti-inflammatory drugs, paracetamol, opioids, anti-convulsant drugs, skeletal muscle relaxants, or corticosteroids) compared with another analgesic medicine, placebo, or no treatment. Adults (≥18 years) who reported acute non-specific low back pain (for less than six weeks).
Data extraction and synthesis: Primary outcomes were low back pain intensity (0-100 scale) at end of treatment and safety (number of participants who reported any adverse event during treatment). Secondary outcomes were low back specific function, serious adverse events, and discontinuation from treatment. Two reviewers independently identified studies, extracted data, and assessed risk of bias. A random effects network meta-analysis was done and confidence was evaluated by the Confidence in Network Meta-Analysis method.
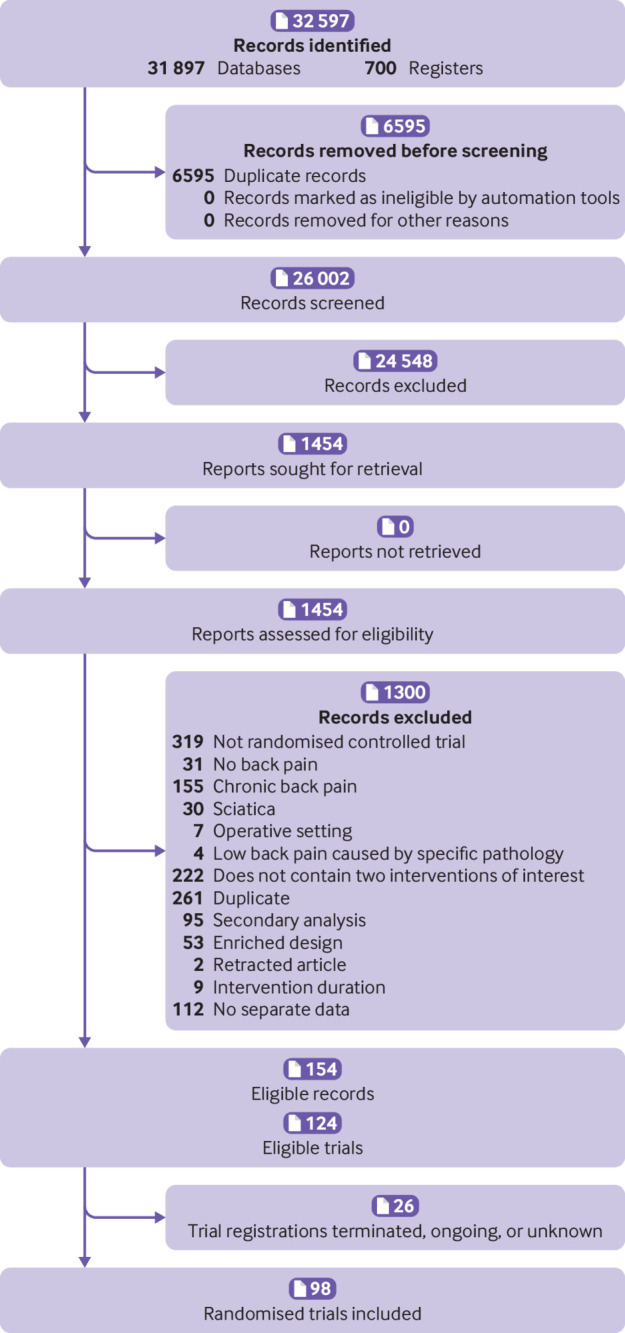
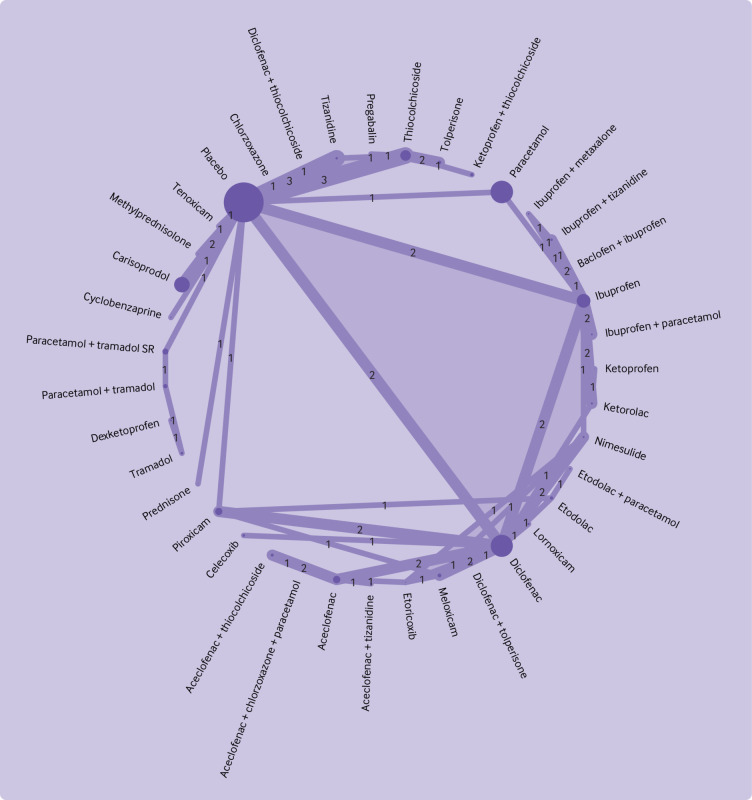
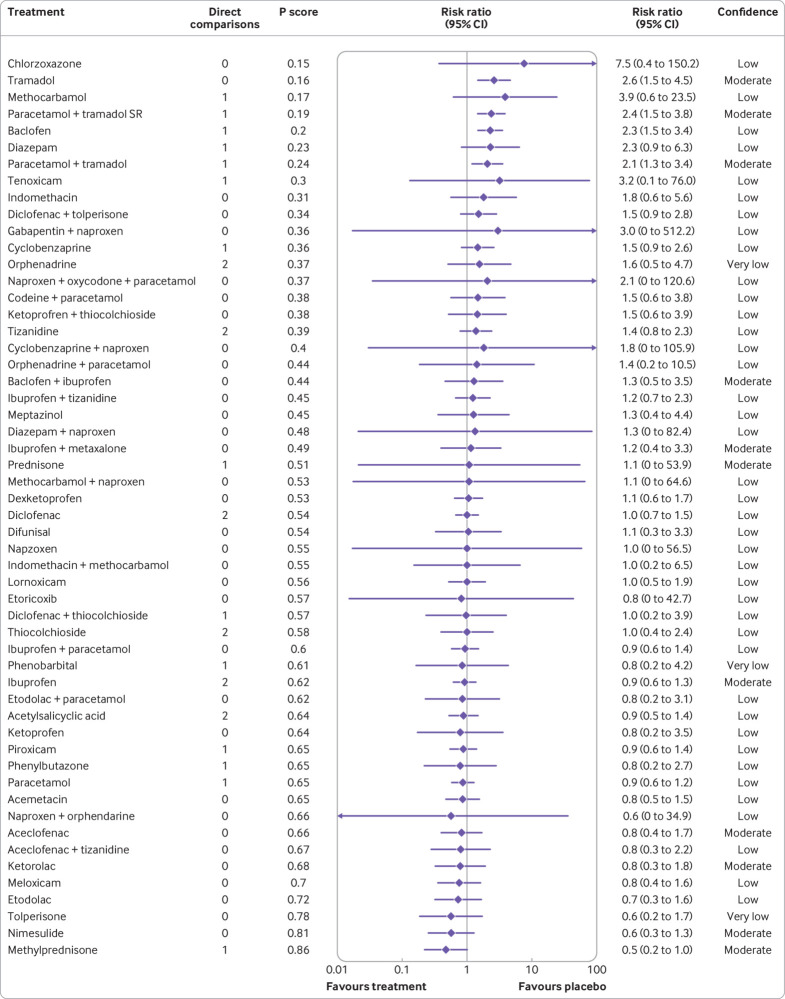
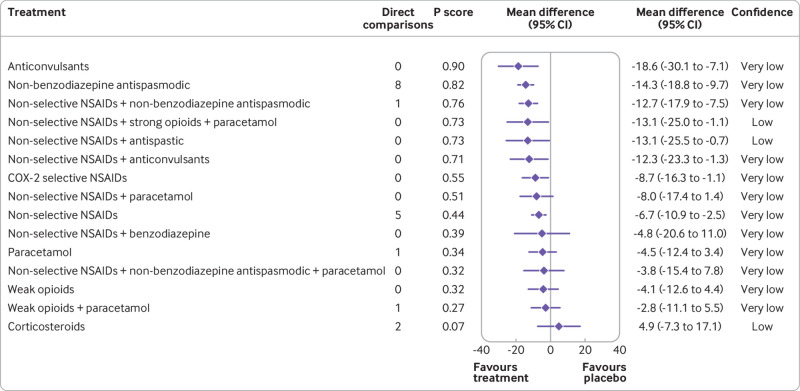
Results: 98 randomised controlled trials (15 134 participants, 49% women) included 69 different medicines or combinations. Low or very low confidence was noted in evidence for reduced pain intensity after treatment with tolperisone (mean difference -26.1 (95% confidence intervals -34.0 to -18.2)), aceclofenac plus tizanidine (-26.1 (-38.5 to -13.6)), pregabalin (-24.7 (-34.6 to -14.7)), and 14 other medicines compared with placebo. Low or very low confidence was noted for no difference between the effects of several of these medicines. Increased adverse events had moderate to very low confidence with tramadol (risk ratio 2.6 (95% confidence interval 1.5 to 4.5)), paracetamol plus sustained release tramadol (2.4 (1.5 to 3.8)), baclofen (2.3 (1.5 to 3.4)), and paracetamol plus tramadol (2.1 (1.3 to 3.4)) compared with placebo. These medicines could increase the risk of adverse events compared with other medicines with moderate to low confidence. Moderate to low confidence was also noted for secondary outcomes and secondary analysis of medicine classes.
Conclusions: The comparative effectiveness and safety of analgesic medicines for acute non-specific low back pain are uncertain. Until higher quality randomised controlled trials of head-to-head comparisons are published, clinicians and patients are recommended to take a cautious approach to manage acute non-specific low back pain with analgesic medicines.
Systematic review registration: PROSPERO CRD42019145257.
© Author(s) (or their employer(s)) 2019. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: All authors have completed the ICMJE uniform disclosure form at https://www.icmje.org/disclosure-of-interest/ and declare: this study received project support funding from a 2020 Exercise Physiology Research (Consumables) Grant from the University of New South Wales, which was used to obtain translations of studies published in languages other than English. MKB received travel support from Memorial University of Newfoundland to speak about engagement with research evidence, including the effects of medicines. The Sydney Pharmacy School receives funding from GlaxoSmithKline for a postgraduate scholarship supporting a research student supervised by AJM; all other authors declare no competing interests.
Figures



References
-
- Qaseem A, Wilt TJ, McLean RM, et al. Clinical Guidelines Committee of the American College of Physicians . Noninvasive treatments for acute, subacute, and chronic low back pain: a clinical practice guideline from the American College of Physicians. Ann Intern Med 2017;166:514-30. 10.7326/M16-2367 - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources