

[Treatment responses, outcomes, and prognostic factors associated with them in patients with secondary acute myeloid leukemia]
- PMID: 36948866
- PMCID: PMC10033265
- DOI: 10.3760/cma.j.issn.0253-2727.2023.02.007
[Treatment responses, outcomes, and prognostic factors associated with them in patients with secondary acute myeloid leukemia]
Abstract
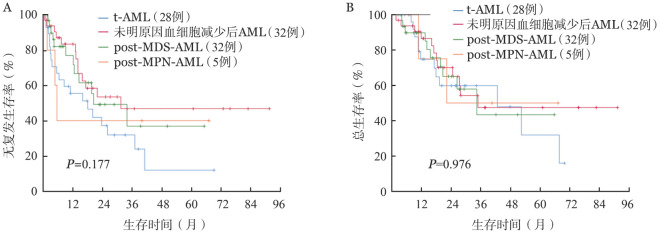
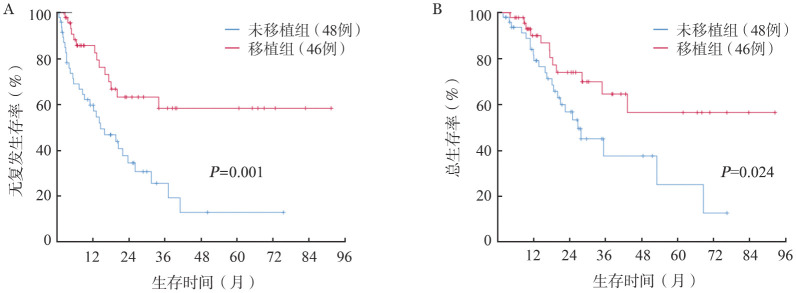
Objective: To evaluate treatment responses, outcomes, and prognostic factors in adults with secondary acute myeloid leukemia (sAML) . Methods: Between January 2008 and February 2021, date of consecutive cases of younger than 65 years of adults with sAML were assessed retrospectively. Clinical characteristics at diagnosis, treatment responses, recurrence, and survival were evaluated. Logistic regression and Cox proportional hazards model were employed to determine significant prognostic indicators for treatment response and survival. Results: 155 patients were recruited, including 38, 46, 57, 14 patients belonging to t-AML, and AML with unexplained cytopenia, post-MDS-AML, and post-MPN-AML, respectively. In the 152 evaluable patients, the rate of MLFS after the initial induction regimen was 47.4%, 57.9%, 54.3%, 40.0%, and 23.1% in the four groups (P=0.076) . The total rate of MLFS after the induction regimen was 63.8%, 73.3%, 69.6%, 58.2%, and 38.5% (P=0.084) , respectively. Multivariate analysis demonstrated that male gender (OR=0.4, 95% CI 0.2-0.9, P=0.038 and OR=0.3, 95% CI 0.1-0.8, P=0.015) , SWOG cytogenetic classification into unfavorable or intermediate (OR=0.1, 95% CI 0.1-0.6, P=0.014 and OR=0.1, 95% CI 0.1-0.3, P=0.004) and receiving low-intensity regimen as induction regimen (OR=0.1, 95% CI 0.1-0.3, P=0.003 and OR=0.1, 95%CI 0.1-0.2, P=0.001) were typical adverse factors impacting the first CR and the final CR; PLT<45 × 10(9)/L (OR=0.4, 95%CI 0.2-0.9, P=0.038) and LDH ≥258 U/L (OR=0.3, 95%CI 0.1-0.7, P=0.005) were independent factors for CR. Among the 94 patients with achieving MLFS, 46 cases had allogeneic hematopoietic stem cell transplantation. With a median follow-up period of 18.6 months, the probabilities of relapse-free survival (RFS) and overall survival (OS) at 3 years were 25.4% and 37.3% in patients with transplantation, and in patients with chemotherapy, the probabilities of RFS and OS at 3-year were 58.2% and 64.3%, respectively. At the time of achieving MLFS, multivariate analysis revealed that age ≥46 years (HR=3.4, 95%CI 1.6-7.2, P=0.002 and HR=2.5, 95%CI 1.1-6.0, P=0.037) , peripheral blasts ≥17.5% at diagnosis (HR=2.5, 95%CI 1.2-4.9, P=0.010 and HR=4.1, 95%CI 1.7-9.7, P=0.002) , monosomal karyotypes (HR=4.9, 95%CI 1.2-19.9, P=0.027 and HR=28.3, 95%CI 4.2-189.5, P=0.001) were typical adverse factors influencing RFS and OS. Furthermore, CR after induction chemotherapy (HR=0.4, 95%CI 0.2-0.8, P=0.015) and transplantation (HR=0.4, 95%CI 0.2-0.9, P=0.028) were substantially linked to longer RFS. Conclusion: Post-MDS-AML and post-MPN-AML had lower response rates and poorer prognoses than t-AML and AML with unexplained cytopenia. In adults with male gender, low platelet count, high LDH, and SWOG cytogenetic classification into unfavorable or intermediate at diagnosis, and receiving low-intensity regimen as the induction regimen predicted a low response rate. Age ≥46 years, a higher proportion of peripheral blasts and monosomal karyotype had a negative effect on the overall outcome. Transplantation and CR after induction chemotherapy were greatly linked to longer RFS.
目的: 探讨成人继发性急性髓系白血病(sAML)的治疗反应和结局及其影响因素。 方法: 回顾性分析2008年1月至2021年2月北京大学人民医院收治的≤65岁sAML的连续病例,包括治疗相关AML(t-AML)、未明原因血细胞减少后AML、继发于骨髓增生异常综合征(MDS)的AML(post-MDS-AML)和继发于骨髓增殖性肿瘤(MPN)的AML(post-MPN-AML)的临床特征、治疗反应、复发和生存,采用二元Logistic模型分析治疗反应影响因素,Cox回归模型分析结局影响因素。 结果: 共纳入155例患者,t-AML、未明原因血细胞减少后AML、post-MDS-AML、post-MPN-AML组分别为38、46、57、14例。152例诱导化疗后可评估疗效患者中,首疗程诱导治疗后形态学无白血病状态(MLFS)率为47.4%,四组分别为57.9%、54.3%、40.0%、23.1%(P=0.076);最终MLFS率为63.8%,四组分别为73.3%、69.6%、58.2%、38.5%(P=0.084)。多因素分析显示,全部患者中,男性(OR=0.4,95%CI 0.2~0.9,P=0.038;OR=0.3,95%CI 0.1~0.8,P=0.015)、SWOG非预后良好组(OR=0.1,95% CI 0.1~0.6,P=0.014;OR=0.1,95%CI 0.1~0.3,P=0.004)以及初始诱导弱化疗(OR=0.1,95%CI 0.1~0.3,P=0.003;OR=0.1,95%CI 0.1~0.2,P=0.001)是不利于首疗程诱导治疗获得完全缓解(CR)及最终获得CR的因素;此外,初诊时PLT<45×10(9)/L(OR=0.4,95%CI 0.2~0.9,P=0.038)、LDH≥258 U/L(OR=0.3,95%CI 0.1~0.7,P=0.005)亦为影响最终获得CR的独立危险因素。94例获得MLFS患者中,46例行异基因造血干细胞移植。中位随访18.6个月,持续化疗患者3年无复发生存(RFS)率和总生存(OS)率分别为25.4%、37.3%,移植患者3年RFS率和OS率分别为58.2%、64.3%。在获得MLFS患者中,多因素分析显示,年龄≥46岁(HR=3.4,95%CI 1.6~7.2,P=0.002;HR=2.5,95%CI 1.1~6.0,P=0.037)、初诊时外周血原始细胞≥17.5%(HR=2.5,95%CI 1.2~4.9,P=0.010;HR=4.1,95%CI 1.7~9.7,P=0.002)、单体核型(HR=4.9,95%CI 1.2~19.9,P=0.027;HR=28.3,95%CI 4.2~189.5,P=0.001)为影响RFS和OS的共同不利因素;此外,首疗程诱导治疗获得CR(HR=0.4,95%CI 0.2~0.8,P=0.015)及接受移植(HR=0.4,95%CI 0.2~0.9,P=0.028)与较长的RFS期显著相关。 结论: 与t-AML和未明原因血细胞减少后AML相比,post-MDS-AML和post-MPN-AML缓解率低、预后差。男性、初诊低PLT、高LDH、SWOG非预后良好组及初始诱导弱化疗是影响成年sAML获得缓解的不利因素,年龄≥46岁、外周血原始细胞比例高、单体核型是影响总体结局的不利因素,移植及诱导缓解达CR与更长的RFS期显著相关。.
Keywords: Early response; Leukemia, myeloid, acute; Prognosis; Secondary leukemia; Survival.
Conflict of interest statement
Figures
Similar articles
-
[Outcomes of adult patients with de novo acute myeloid leukemia received idarubicin plus cytarabine regimen as induction chemotherapy].Zhonghua Xue Ye Xue Za Zhi. 2018 Jan 14;39(1):15-21. doi: 10.3760/cma.j.issn.0253-2727.2018.01.004. Zhonghua Xue Ye Xue Za Zhi. 2018. PMID: 29551027 Free PMC article. Chinese.
-
[Factors associated with early treatment response in adults with acute myeloid leukemia].Zhonghua Xue Ye Xue Za Zhi. 2017 Oct 14;38(10):869-875. doi: 10.3760/cma.j.issn.0253-2727.2017.10.009. Zhonghua Xue Ye Xue Za Zhi. 2017. PMID: 29166740 Free PMC article. Chinese.
-
[Prognostic significance of early assessment of minimal residual disease in acute myeloid leukemia with mutated NPM1 patients].Zhonghua Xue Ye Xue Za Zhi. 2017 Jan 14;38(1):10-16. doi: 10.3760/cma.j.issn.0253-2727.2017.01.003. Zhonghua Xue Ye Xue Za Zhi. 2017. PMID: 28219218 Free PMC article. Chinese.
-
The prognostic value of cytogenetics is reinforced by the kind of induction/consolidation therapy in influencing the outcome of acute myeloid leukemia--analysis of 848 patients.Leukemia. 2001 Jun;15(6):903-9. doi: 10.1038/sj.leu.2402142. Leukemia. 2001. PMID: 11417475 Review.
-
Comparing Hematopoietic Cell Transplant versus Other Treatments for Adults with Acute Myeloid Leukemia [Internet].Washington (DC): Patient-Centered Outcomes Research Institute (PCORI); 2021 Jan. Washington (DC): Patient-Centered Outcomes Research Institute (PCORI); 2021 Jan. PMID: 38232198 Free Books & Documents. Review.
References
-
- Slovak ML, Kopecky KJ, Cassileth PA, et al. Karyotypic analysis predicts outcome of preremission and postremission therapy in adult acute myeloid leukemia: a Southwest Oncology Group/Eastern Cooperative Oncology Group Study[J] Blood. 2000;96(13):4075–4083. - PubMed
-
- Zhao XS, Qin YZ, Liu YR, et al. The impact of minimal residual disease prior to unmanipulated haploidentical hematopoietic stem cell transplantation in patients with acute myeloid leukemia in complete remission[J] Leuk Lymphoma. 2017;58(5):1135–1143. doi: 10.1080/10428194.2016.1239264. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous