

Correlates of protection and viral load trajectories in omicron breakthrough infections in triple vaccinated healthcare workers
- PMID: 36949041
- PMCID: PMC10031702
- DOI: 10.1038/s41467-023-36984-1
Correlates of protection and viral load trajectories in omicron breakthrough infections in triple vaccinated healthcare workers
Abstract
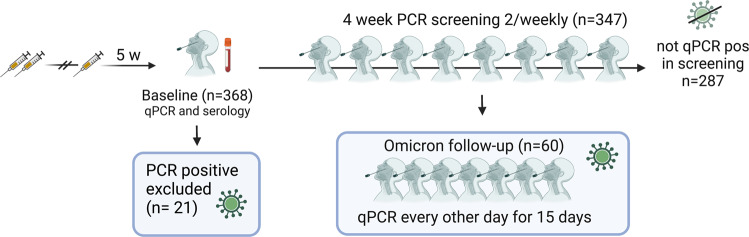
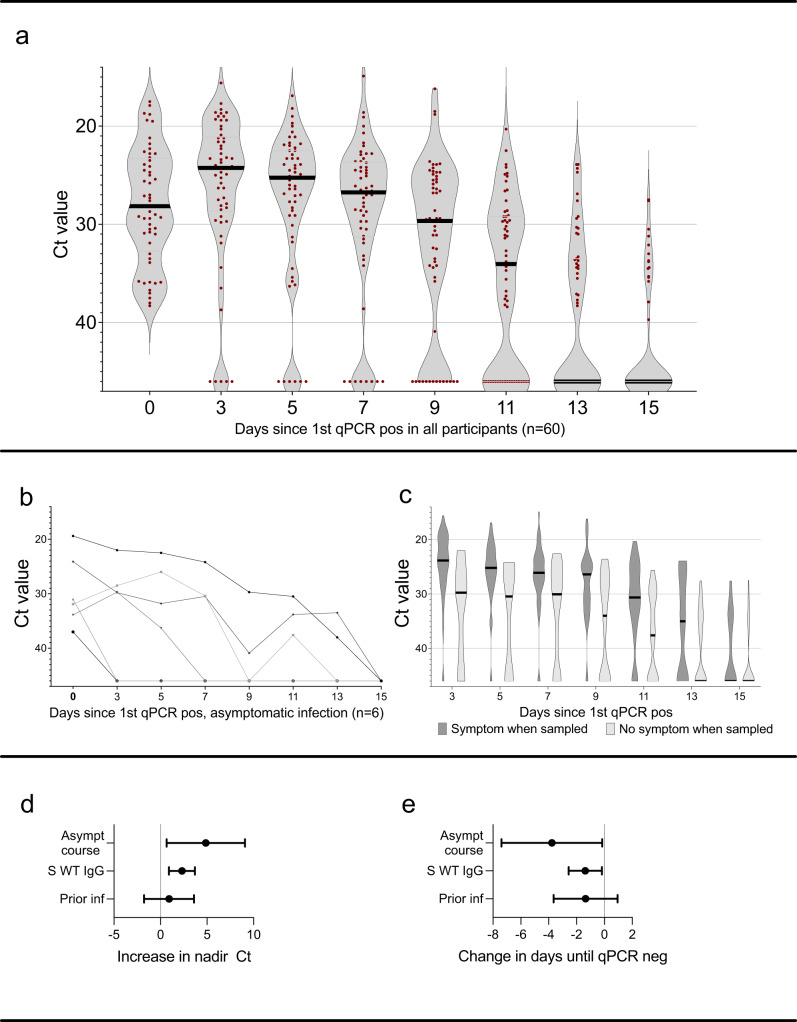
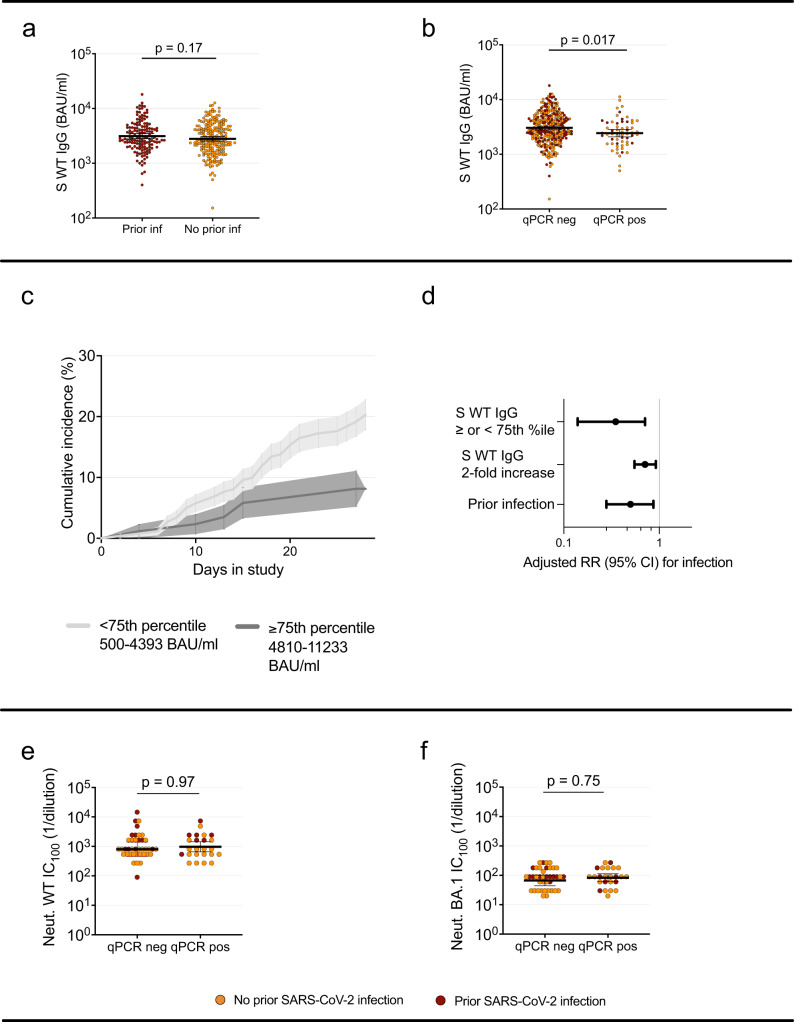
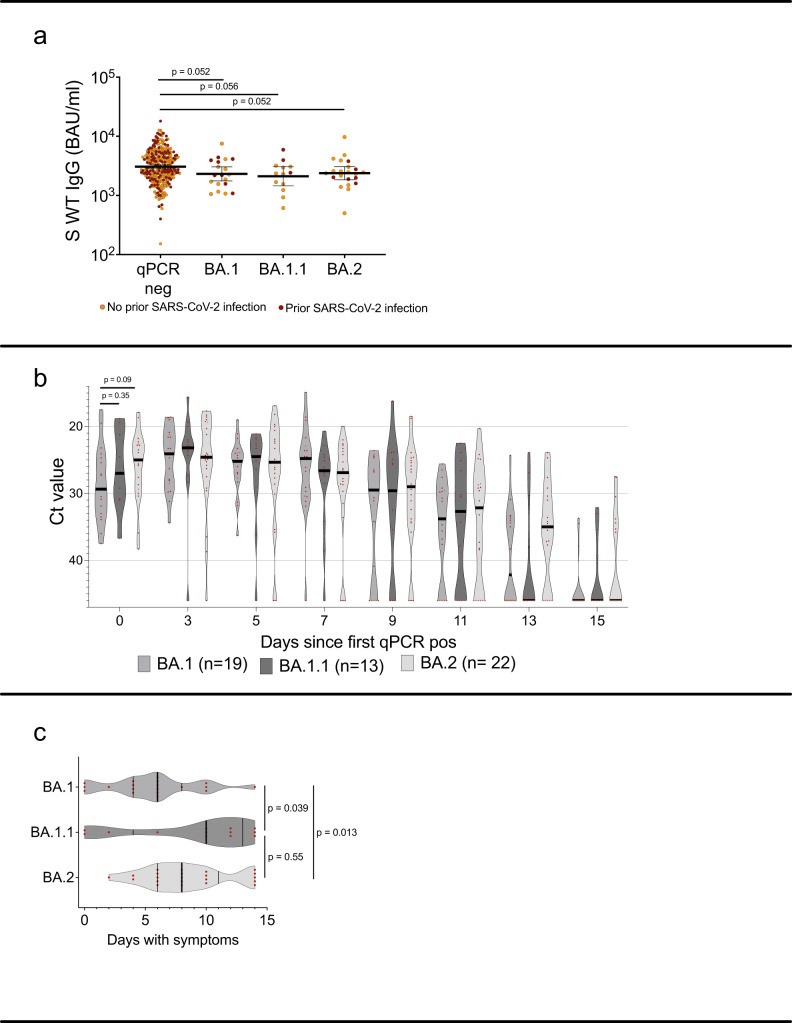
Vaccination offers protection against severe COVID-19 caused by SARS-CoV-2 omicron but is less effective against infection. Characteristics such as serum antibody titer correlation to protection, viral abundance and clearance of omicron infection in vaccinated individuals are scarce. We present a 4-week twice-weekly SARS-CoV-2 qPCR screening in 368 triple vaccinated healthcare workers. Spike-specific IgG levels, neutralization titers and mucosal spike-specific IgA-levels were determined at study start and qPCR-positive participants were sampled repeatedly for two weeks. 81 (cumulative incidence 22%) BA.1, BA.1.1 and BA.2 infections were detected. High serum antibody titers are shown to be protective against infection (p < 0.01), linked to reduced viral load (p < 0.01) and time to viral clearance (p < 0.05). Pre-omicron SARS-CoV-2 infection is independently associated to increased protection against omicron, largely mediated by mucosal spike specific IgA responses (nested models lr test p = 0.02 and 0.008). Only 10% of infected participants remain asymptomatic through the course of their infection. We demonstrate that high levels of vaccine-induced spike-specific WT antibodies are linked to increased protection against infection and to reduced viral load if infected, and suggest that the additional protection offered by pre-omicron SARS-CoV-2 infection largely is mediated by mucosal spike-specific IgA.
© 2023. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- Lyngse, F.P. et al. SARS-CoV-2 Omicron VOC Transmission in Danish Households. medRxiv. 2021.2012.2027.21268278 (2021).
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
