

Statin protects men but not women with HIV against loss of muscle mass, strength, and physical function: a pilot study
- PMID: 36949103
- PMCID: PMC10033712
- DOI: 10.1038/s41598-023-31643-3
Statin protects men but not women with HIV against loss of muscle mass, strength, and physical function: a pilot study
Abstract
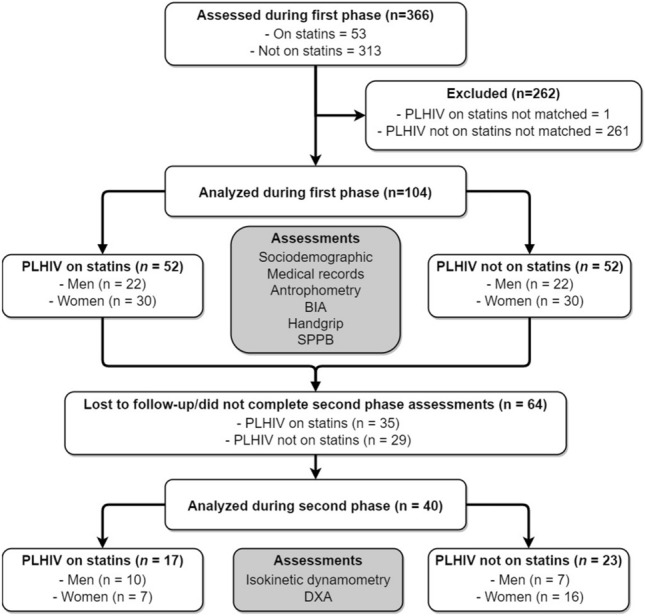
Statins are cholesterol-lowering drugs commonly used among people with HIV, associated with an increased risk of myopathies. Considering that cardiovascular disease, statin therapy, and sarcopenia are independently prevalent in people with HIV, clarity on the potential benefits or harms of statin therapy on muscle health is useful to provide insight into ways to maximize skeletal muscle health and minimize CVD risk in this population. We aimed to study the effects of statin therapy on strength, muscle mass, and physical function parameters in people with HIV. This was a pilot cross-sectional study. People with HIV on continuous statin therapy (n = 52) were paired 1:1 according to age (people with HIV 53.9 ± 8.2 and people with HIV on statins 53.9 ± 8.4 years), sex, body mass index (Body mass index, people with HIV 28.6 ± 5.3 and people with HIV on statins 28.8 ± 6.3 kg/m2), and race with people with HIV not using statin (n = 52). Participants were evaluated for muscle strength (i.e. handgrip strength), lean and fat body mass (using bioelectric impedance analysis), and physical function (i.e. Short Physical Performance Battery-SPPB). Isokinetic strength and appendicular lean mass (using dual-energy X-ray absorptiometry), more accurate strength and body composition measures, were determined in 38% of the participants. Overall, statin usage does not exacerbated loss of muscle strength (32.2 ± 11.5 vs. 30.3 ± 9.6 kg, p > 0.05) muscle mass (7.6 ± 1.8 vs. 7.7 ± 1.1 kg/m2, p > 0.05), and impaired physical performance (10.1 ± 1.8 vs. 9.7 ± 2.1 points, p > 0.05) of PLWH. When analyzed by sex, men living with HIV on statins usage presented higher appendicular muscle mass (28.4 ± 3.1 vs. 26.2 ± 4.9 kg, p < 0.05) handgrip strength (42.1 ± 8.8 vs. 37.1 ± 8.3 kg, p < 0.05) and physical function through SPPB score (10.9 ± 1.3 vs. 9.5 ± 2.1, p < 0.05) than men living with HIV not on statins treatment. The same protection was not observed in women. This data was demonstrated when muscle mass and strength were determined clinically (i.e. handgrip strength and electrical impedance) and when more precise laboratory measurements of muscle mass and strength were conducted (i.e. isokinetic strength and DXA scans). Statin does not exacerbate muscle wasting, strength loss, or muscle dysfunction among people with HIV. Indeed, statins may protect men, but not woman with HIV against HIV and antiretroviral therapy-induced loss of muscle mass and strength.
© 2023. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures

References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
