

Guidelines for Neuroprognostication in Comatose Adult Survivors of Cardiac Arrest
- PMID: 36949360
- PMCID: PMC10241762
- DOI: 10.1007/s12028-023-01688-3
Guidelines for Neuroprognostication in Comatose Adult Survivors of Cardiac Arrest
Abstract
Background: Among cardiac arrest survivors, about half remain comatose 72 h following return of spontaneous circulation (ROSC). Prognostication of poor neurological outcome in this population may result in withdrawal of life-sustaining therapy and death. The objective of this article is to provide recommendations on the reliability of select clinical predictors that serve as the basis of neuroprognostication and provide guidance to clinicians counseling surrogates of comatose cardiac arrest survivors.
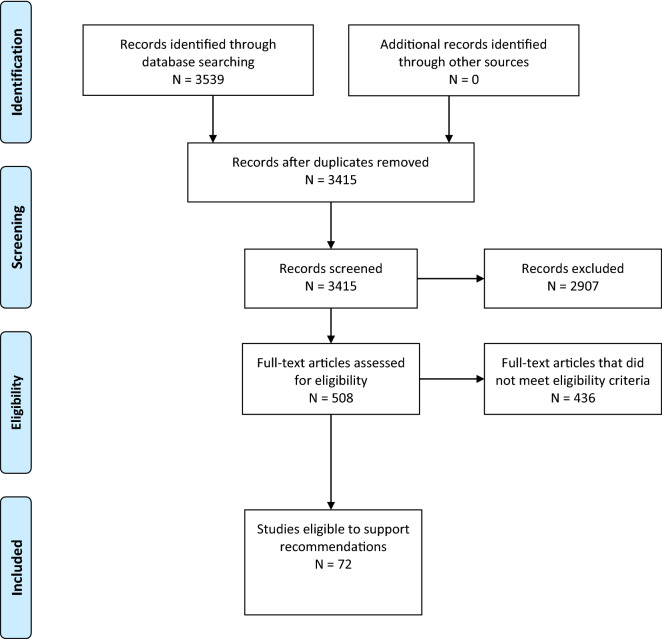
Methods: A narrative systematic review was completed using Grading of Recommendations Assessment, Development and Evaluation (GRADE) methodology. Candidate predictors, which included clinical variables and prediction models, were selected based on clinical relevance and the presence of an appropriate body of evidence. The Population, Intervention, Comparator, Outcome, Timing, Setting (PICOTS) question was framed as follows: "When counseling surrogates of comatose adult survivors of cardiac arrest, should [predictor, with time of assessment if appropriate] be considered a reliable predictor of poor functional outcome assessed at 3 months or later?" Additional full-text screening criteria were used to exclude small and lower-quality studies. Following construction of the evidence profile and summary of findings, recommendations were based on four GRADE criteria: quality of evidence, balance of desirable and undesirable consequences, values and preferences, and resource use. In addition, good practice recommendations addressed essential principles of neuroprognostication that could not be framed in PICOTS format.
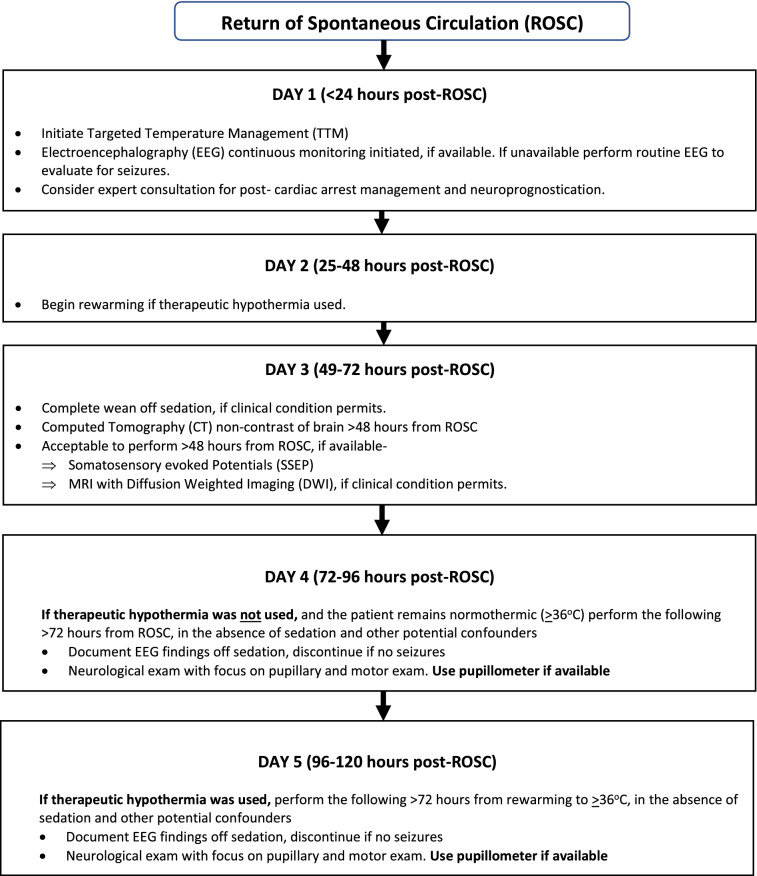
Results: Eleven candidate clinical variables and three prediction models were selected based on clinical relevance and the presence of an appropriate body of literature. A total of 72 articles met our eligibility criteria to guide recommendations. Good practice recommendations include waiting 72 h following ROSC/rewarming prior to neuroprognostication, avoiding sedation or other confounders, the use of multimodal assessment, and an extended period of observation for awakening in patients with an indeterminate prognosis, if consistent with goals of care. The bilateral absence of pupillary light response > 72 h from ROSC and the bilateral absence of N20 response on somatosensory evoked potential testing were identified as reliable predictors. Computed tomography or magnetic resonance imaging of the brain > 48 h from ROSC and electroencephalography > 72 h from ROSC were identified as moderately reliable predictors.
Conclusions: These guidelines provide recommendations on the reliability of predictors of poor outcome in the context of counseling surrogates of comatose survivors of cardiac arrest and suggest broad principles of neuroprognostication. Few predictors were considered reliable or moderately reliable based on the available body of evidence.
Keywords: Cardiac arrest; Coma; Functional status; Mortality; Prognosis.
© 2023. The Author(s).
Conflict of interest statement
None of the authors have any conflicts to disclose related to the content of this manuscript.
Figures

References
-
- Cardiac Arrest Registry to Enhance Survival (CARES) 2020 annual report. 2020 [cited 2021 November 17 2021]. https://mycares.net/sitepages/uploads/2021/2020_flipbook/index.html?page=1.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
