

Evaluation of Cannulated Compression Headless Screw (CCHS) as an alternative implant in comparison to standard S1-S2 screw fixation of the posterior pelvis ring: a biomechanical study
- PMID: 36949409
- PMCID: PMC10035201
- DOI: 10.1186/s12891-023-06312-1
Evaluation of Cannulated Compression Headless Screw (CCHS) as an alternative implant in comparison to standard S1-S2 screw fixation of the posterior pelvis ring: a biomechanical study
Abstract
Background/purpose: Posterior pelvis ring injuries represent typical high-energy trauma injuries in young adults. Joint stabilization with two cannulated sacroiliac (SI) screws at the level of sacral vertebrae S1 and S2 is a well-established procedure. However, high failure- and implant removal (IR) rates have been reported. Especially, the washer recovery can pose the most difficult part of the IR surgery, which is often associated with complications. The aim of this biomechanical study was to evaluate the stability of S1-S2 fixation of the SI joint using three different screw designs.
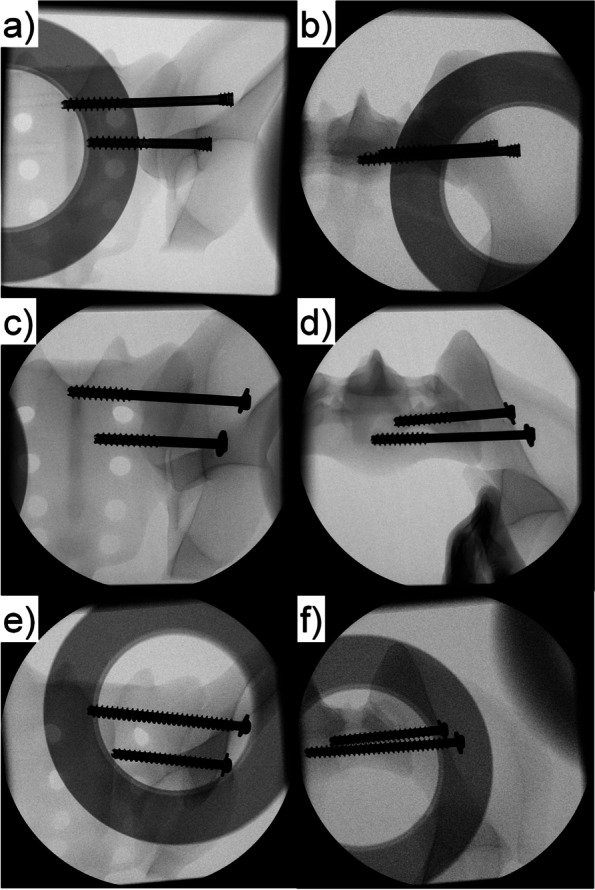
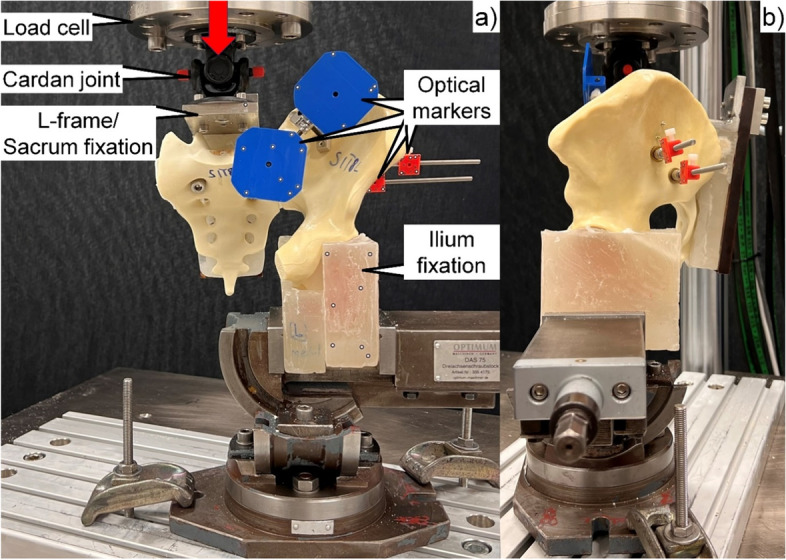
Methods: Eighteen artificial hemi-pelvises were assigned to three groups (n = 6) for SI joint stabilization through S1 and S2 corridors using either two 7.5 mm cannulated compression headless screws (group CCH), two 7.3 mm partially threaded SI screws (group PT), or two 7.3 mm fully threaded SI screws (group FT). An SI joint dislocation injury type III APC according to the Young and Burgess classification was simulated before implantation. All specimens were biomechanically tested to failure in upright standing position under progressively increasing cyclic loading. Interfragmentary and bone-implant movements were captured via motion tracking and evaluated at four time points between 4000 and 7000 cycles.
Results: Combined interfragmentary angular displacement movements in coronal and transverse plane between ilium and sacrum, evaluated over the measured four time points, were significantly bigger in group FT versus both groups CCH and PT, p ≤ 0.047. In addition, angular displacement of the screw axis within the ilium under consideration of both these planes was significantly bigger in group FT versus group PT, p = 0.038. However, no significant differences were observed among the groups for screw tip cutout movements in the sacrum, p = 0.321. Cycles to failure were highest in group PT (9885 ± 1712), followed by group CCH (9820 ± 597), and group FT (7202 ± 1087), being significantly lower in group FT compared to both groups CCH and PT, p ≤ 0.027.
Conclusion: From a biomechanical perspective, S1-S2 SI joint fixation using two cannulated compression headless screws or two partially threaded SI screws exhibited better interfragmentary stability compared to two fully threaded SI screws. The former can therefore be considered as a valid alternative to standard SI screw fixation in posterior pelvis ring injuries. In addition, partially threaded screw fixation was associated with less bone-implant movements versus fully threaded screw fixation. Further human cadaveric biomechanical studies with larger sample size should be initiated to understand better the potential of cannulated compression headless screw fixation for the therapy of the injured posterior pelvis ring in young trauma patients.
Keywords: Biomechanics; Cannulated Compression Headless Screw; Posterior pelvis ring injuries; Sacroiliac joint disruption.
© 2023. The Author(s).
Conflict of interest statement
None of the authors have any conflicts of interest to declare.
Figures

References
-
- Starr AJ, Walter JC, Harris RW, Reinert CM, Jones AL. Percutaneous screw fixation of fractures of the iliac wing and fracture-dislocations of the sacro-iliac joint (OTA Types 61–B2. 2 and 61–B2. 3, or Young-Burgess “lateral compression type II” pelvic fractures) J Orthop Trauma. 2002;16(2):116–23. doi: 10.1097/00005131-200202000-00008. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
