

An update on the management of non-variceal upper gastrointestinal bleeding
- PMID: 36949934
- PMCID: PMC10027415
- DOI: 10.1093/gastro/goad011
An update on the management of non-variceal upper gastrointestinal bleeding
Abstract
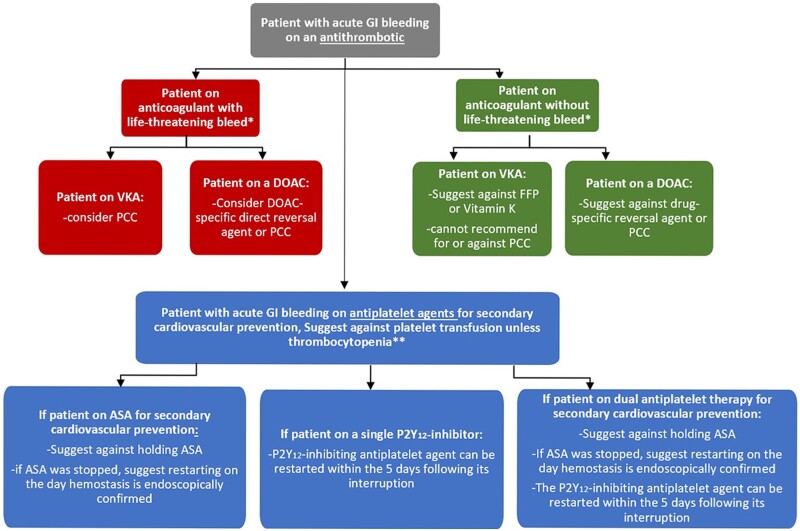
Upper gastrointestinal bleeding (UGIB) continues to be a common gastrointestinal emergency that carries significant morbidity and mortality. The epidemiology of UGIB has been changing over the last few decades with an overall decrease in peptic ulcer disease and increase in the prevalence of other etiologies including vascular lesions and malignancy. Appropriate risk assessment and patient stratification are crucial to ensuring that optimal care is delivered to patients and some risk assessment tools have shown excellent ability to define a low-risk group who can be managed as outpatients safely. Regardless of the etiology of UGIB, resuscitative interventions by primary care providers remain the most important initial measures to improve the outcome for patients including hemodynamic stabilization, an appropriate blood transfusion strategy, with or without acid-lowering agents, while also providing subsequent urgent endoscopic assessment and intervention. In addition, with increasing use of antithrombotic agents in clinical practice and its associated risk of bleeding, the management of such agents in the acute setting has become a real challenge to all physicians. In this article, we provide an up-to-date, evidence-based, practical review of recent changes and advances in UGIB with a focus on non-variceal etiologies.
Keywords: UGIB; antithrombotic; endoscopic hemostasis; peptic ulcer; risk assessment.
© The Author(s) 2023. Published by Oxford University Press and Sixth Affiliated Hospital of Sun Yat-sen University.
Conflict of interest statement
None declared.
Figures




References
-
- Abougergi MS, Travis AC, Saltzman JR.. The in-hospital mortality rate for upper GI hemorrhage has decreased over 2 decades in the United States: a nationwide analysis. Gastrointest Endosc 2015;81:882–8.e1. - PubMed
-
- Patel SD, Desai R, Patel U. et al. Thirty-day readmissions after upper and lower gastrointestinal hemorrhage: a national perspective in the United States. J Clin Gastroenterol 2019;53:582–90. - PubMed
-
- Wuerth BA, Rockey DC.. Changing epidemiology of upper gastrointestinal hemorrhage in the last decade: a nationwide analysis. Dig Dis Sci 2018;63:1286–93. - PubMed
-
- Gupta A, Agarwal R, Ananthakrishnan AN.. “Weekend effect” in patients with upper gastrointestinal hemorrhage: a systematic review and meta-analysis. Am J Gastroenterol 2018;113:13–21. - PubMed
-
- van Leerdam ME. Epidemiology of acute upper gastrointestinal bleeding. Best Pract Res Clin Gastroenterol 2008;22:209–24. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
