

Lifetime quality-adjusted life years lost due to genital herpes acquired in the United States in 2018: a mathematical modeling study
- PMID: 36950038
- PMCID: PMC10025423
- DOI: 10.1016/j.lana.2023.100427
Lifetime quality-adjusted life years lost due to genital herpes acquired in the United States in 2018: a mathematical modeling study
Abstract
Background: Genital herpes (GH), caused by herpes simplex virus type 1 and type 2 (HSV-1, HSV-2), is a common sexually transmitted disease associated with adverse health outcomes. Symptoms associated with GH outbreaks can be reduced by antiviral medications, but the infection is incurable and lifelong. In this study, we estimate the long-term health impacts of GH in the United States using quality-adjusted life years (QALYs) lost.
Methods: We used probability trees to model the natural history of GH secondary to infection with HSV-1 and HSV-2 among people aged 18-49 years. We modelled the following outcomes to quantify the major causes of health losses following infection: symptomatic herpes outbreaks, psychosocial impacts associated with diagnosis and recurrences, urinary retention caused by sacral radiculitis, aseptic meningitis, Mollaret's meningitis, and neonatal herpes. The model was parameterized based on published literature on the natural history of GH. We summarized losses of health by computing the lifetime number of QALYs lost per genital HSV-1 and HSV-2 infection, and we combined this information with incidence estimates to compute the total lifetime number of QALYs lost due to infections acquired in 2018 in the United States.
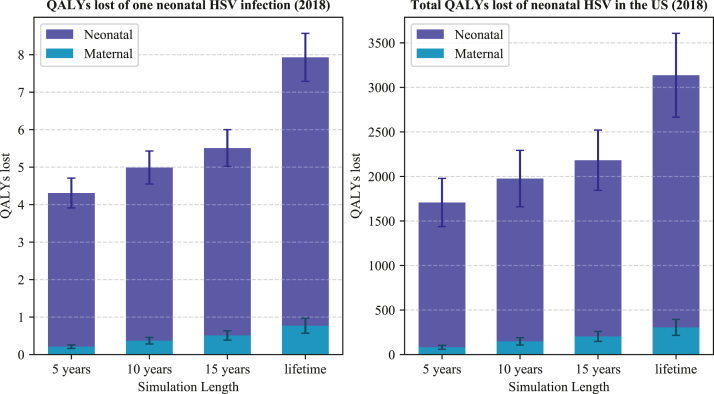
Findings: We estimated 0.05 (95% uncertainty interval (UI) 0.02-0.08) lifetime QALYs lost per incident GH infection acquired in 2018, equivalent to losing 0.05 years or about 18 days of life for one person with perfect health. The average number of QALYs lost per GH infection due to genital HSV-1 and HSV-2 was 0.01 (95% UI 0.01-0.02) and 0.05 (95% UI 0.02-0.09), respectively. The burden of genital HSV-1 is higher among women, while the burden of HSV-2 is higher among men. QALYs lost per neonatal herpes infection was estimated to be 7.93 (95% UI 6.63-9.19). At the population level, the total estimated lifetime QALYs lost as a result of GH infections acquired in 2018 was 33,100 (95% UI 12,600-67,900) due to GH in adults and 3,140 (95% UI 2,260-4,140) due to neonatal herpes. Results were most sensitive to assumptions on the magnitude of the disutility associated with post-diagnosis psychosocial distress and symptomatic recurrences.
Interpretation: GH is associated with substantial health losses in the United States. Results from this study can be used to compare the burden of GH to other diseases, and it provides inputs that may be used in studies on the health impact and cost-effectiveness of interventions that aim to reduce the burden of GH.
Funding: The Center for Disease Control and Prevention.
Keywords: Burden of disease; Economic modeling; Genital herpes; Genital ulcer disease; HSV-1; HSV-2; Herpes simplex virus; Neonatal herpes; Probability tree; Quality-adjusted life years; Sexually transmitted disease.
© 2023 The Author(s).
Conflict of interest statement
MMR reports contract for work on cervical cancer elimination modeling in South Africa, not related to the manuscript, from World Health Organization, travel and lodging support for attending a research project meeting at the World Health Organization headquarters in Geneva, Switzerland, not related to the manuscript, from World Health Organization. YL reports postdoctoral fellowship stipend (2020–2022) from Harvard T. H. Chan School of Public Health, not related to the manuscript. SY reports doctoral stipend from New York University Grossman School of Medicine, not related to the manuscript. All other authors report no potential conflicts.
Figures






Similar articles
-
The Estimated Lifetime Quality-Adjusted Life-Years Lost Due to Chlamydia, Gonorrhea, and Trichomoniasis in the United States in 2018.J Infect Dis. 2023 Apr 18;227(8):1007-1018. doi: 10.1093/infdis/jiad047. J Infect Dis. 2023. PMID: 36806950 Free PMC article.
-
Estimated economic burden of genital herpes and HIV attributable to herpes simplex virus type 2 infections in 90 low- and middle-income countries: A modeling study.PLoS Med. 2022 Dec 15;19(12):e1003938. doi: 10.1371/journal.pmed.1003938. eCollection 2022 Dec. PLoS Med. 2022. PMID: 36520853 Free PMC article.
-
Estimated global and regional incidence and prevalence of herpes simplex virus infections and genital ulcer disease in 2020: mathematical modelling analyses.Sex Transm Infect. 2025 May 19;101(4):214-223. doi: 10.1136/sextrans-2024-056307. Sex Transm Infect. 2025. PMID: 39658199 Free PMC article.
-
Estimation of the Lifetime Quality-Adjusted Life Years (QALYs) Lost Due to Syphilis Acquired in the United States in 2018.Clin Infect Dis. 2023 Feb 8;76(3):e810-e819. doi: 10.1093/cid/ciac427. Clin Infect Dis. 2023. PMID: 35684943 Free PMC article.
-
Estimated costs and quality-adjusted life-years lost due to N. gonorrhoeae infections acquired in 2015 in the United States: A modelling study of overall burden and disparities by age, race/ethnicity, and other factors.Lancet Reg Health Am. 2022 Sep 5;16:100364. doi: 10.1016/j.lana.2022.100364. eCollection 2022 Dec. Lancet Reg Health Am. 2022. PMID: 36777156 Free PMC article.
Cited by
-
Novel Adjuvant S-540956 Targets Lymph Nodes and Reduces Genital Recurrences and Vaginal Shedding of HSV-2 DNA When Administered with HSV-2 Glycoprotein D as a Therapeutic Vaccine in Guinea Pigs.Viruses. 2023 May 10;15(5):1148. doi: 10.3390/v15051148. Viruses. 2023. PMID: 37243234 Free PMC article.
-
The Impacts and Consequences of Sexually Transmitted Infections in the United States.Sex Transm Dis. 2025 May 1;52(5):285-289. doi: 10.1097/OLQ.0000000000002126. Epub 2024 Dec 23. Sex Transm Dis. 2025. PMID: 39714030 Review.
References
-
- Tunkel A.R. In: Aseptic meningitis in adults. Martin S., Hirsch J.M., editors. UpToDate; 2022.
Grants and funding
LinkOut - more resources
Full Text Sources
