

Implications of the paradigm shift in management of Helicobacter pylori infections
- PMID: 36950252
- PMCID: PMC10026128
- DOI: 10.1177/17562848231160858
Implications of the paradigm shift in management of Helicobacter pylori infections
Abstract
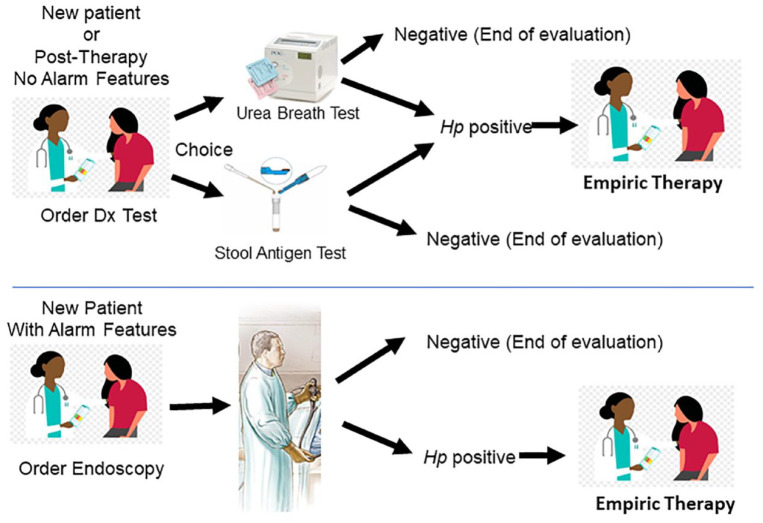
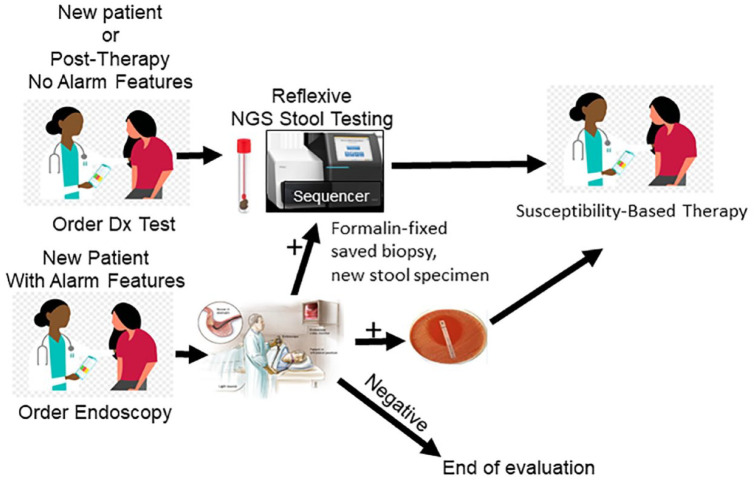
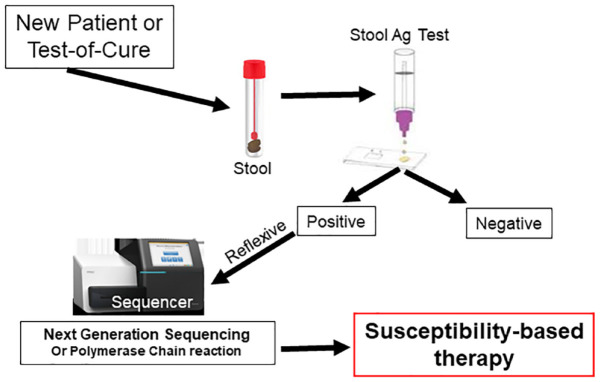
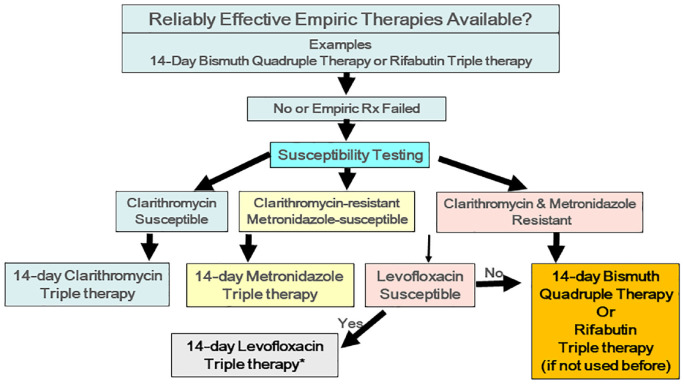
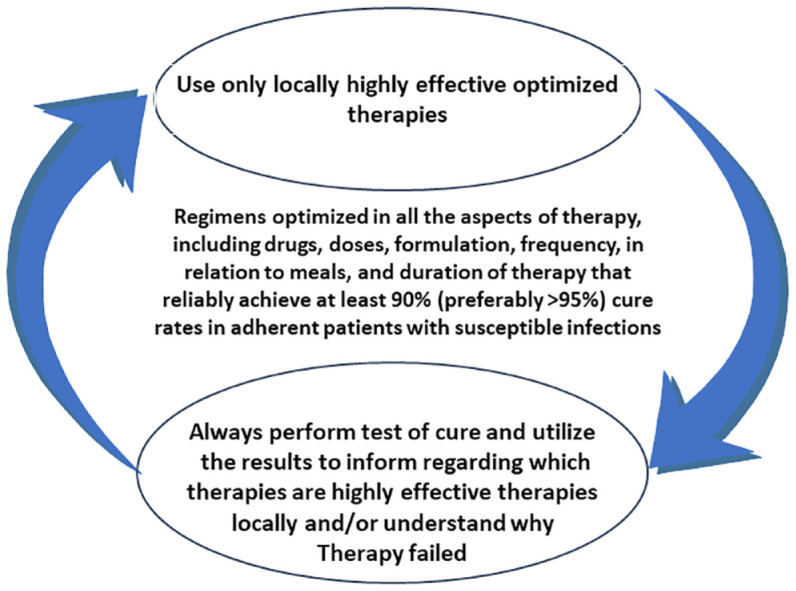
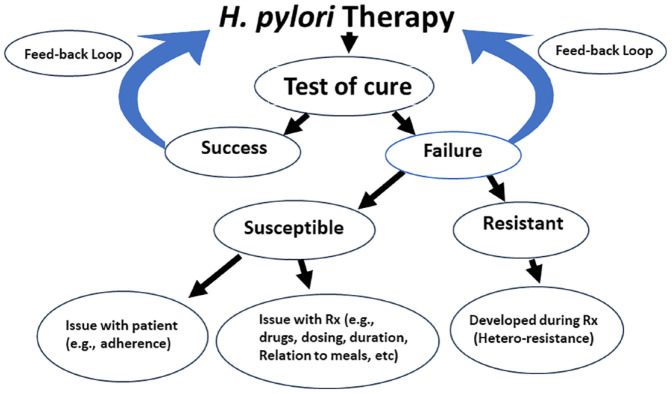
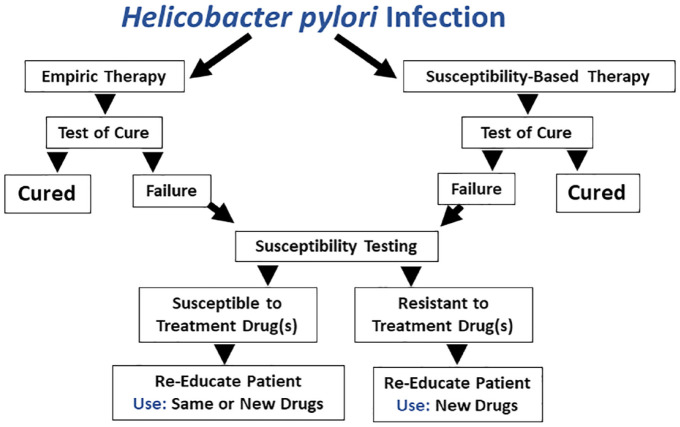
The recent availability of susceptibility testing for Helicobacter pylori infections in the United Sates has resulted in paradigm shifts in the diagnosis, therapy, and follow-up of H. pylori infections. Here, we reviewed the English literature concerning changes in H. pylori diagnosis and therapy with an emphasis on the last 3 years. We focus on the new methods that offer rapid and convenient susceptibility testing using either invasive (endoscopic) or noninvasive (stool) methods of obtaining test material. We also discuss the implications of this availability on therapy and follow-up after therapy. The approach to therapy was categorized into four groups: (1) therapies that can be used empirically, (2) therapies that should be restricted to those that are susceptibility-based, (3) potentially effective therapies that have yet to be optimized for local use, and (4), therapies that contain unneeded antibiotics that should not be prescribed. The most convenient and efficient method of susceptibility testing is by using reflexive stool testing in which if the sample is positive, it is automatically also used for determination of susceptibility. Reflexive testing can also be done via reflexive ordering (e.g., for all positive urea breath tests). The post therapy test-of-cure has emerged as a critical component of therapy as it not only provides feedback regarding treatment success but when combined with susceptibility testing also provide evidence regarding the cause of failure (e.g., poor adherence versus emergence of resistance during therapy. Susceptibility testing has made even the most current H. pylori guidelines for diagnosis and therapy generally obsolete. Clarithromycin, metronidazole, and levofloxacin triple therapies should only be administered as susceptibility-based therapy. Regimens containing unneeded antibiotics should not be given. We provide recommendations regarding the details and indications for all current therapies.
Keywords: Helicobacter pylori; heteroresistance; molecular stool testing; optimization; paradigm shift; susceptibility testing; test-of-cure; treatment; treatment failure; treatment guidelines.
© The Author(s), 2023.
Conflict of interest statement
Dr David Y. Graham is a consultant for RedHill Biopharma and Phathom Pharmaceuticals regarding novel Helicobacter pylori therapies and has received research support for culture of H. pylori. He is also a consultant with Janssen Research & Development regarding potential gastrointestinal effects of drugs under development and has collaborated on research projects with American Molecular regarding molecular diagnostics for H. pylori.
Figures
References
-
- Borsch GM, Graham DY. Helicobacter pylori. In: Collen MJ, Benjamin SB. (eds) Pharmacology of peptic ulcer disease, handbook of experimental pharmacology. Vol 99. Berlin: Springer-Verlag, 1991, pp.107–148.
-
- Hurst AF. Schorstein lecture on the precursors of carcinoma of the stomach. Lancet 1929: 214: 1023–1028.