

Micronutrient Supplementation and Bone Health After Prophylactic Total Gastrectomy in Patients With CDH1 Variants
- PMID: 36950857
- PMCID: PMC10505525
- DOI: 10.1210/clinem/dgad137
Micronutrient Supplementation and Bone Health After Prophylactic Total Gastrectomy in Patients With CDH1 Variants
Abstract
Introduction: Patients with germline variants in CDH1 who undergo prophylactic total gastrectomy (TG) are at risk of altered nutrient and drug absorption due to modified gastrointestinal anatomy. Bone mineral density loss and micronutrient deficiencies have not been described previously in this patient population.
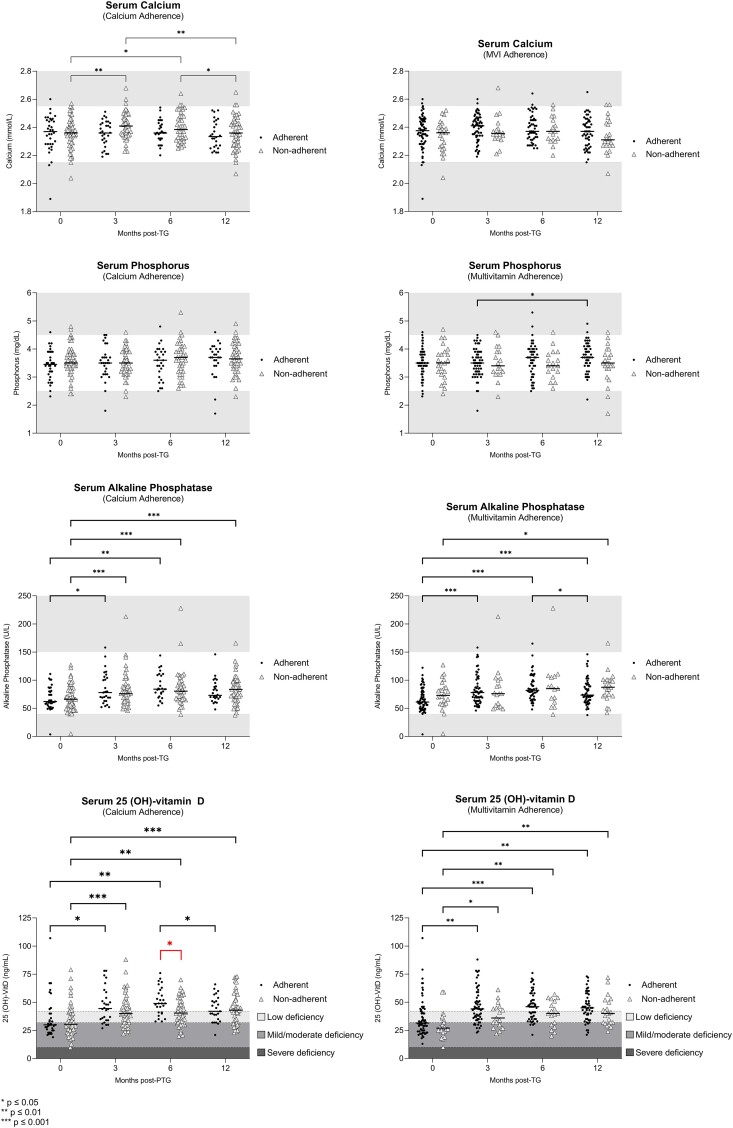
Methods: In this study we included 94 patients with germline CDH1 variants who underwent prophylactic TG between October 2017 and February 2022. We examined pre- and post-gastrectomy bone mineral density (BMD); serum biomarkers including calcium, phosphorus, alkaline phosphatase, and 25 (OH)-vitamin D; and postoperative adherence to calcium and multivitamin supplementation.
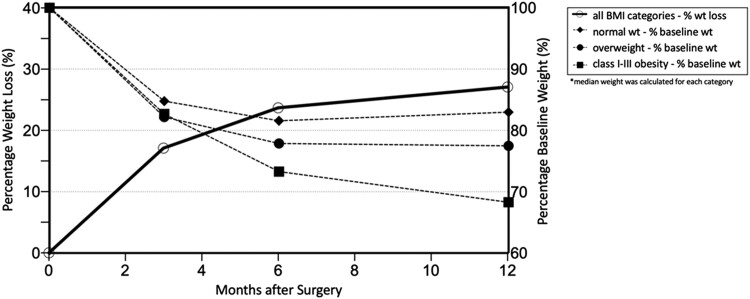
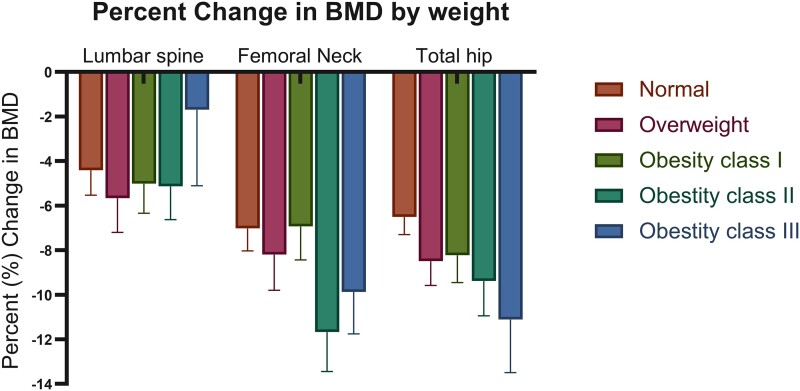
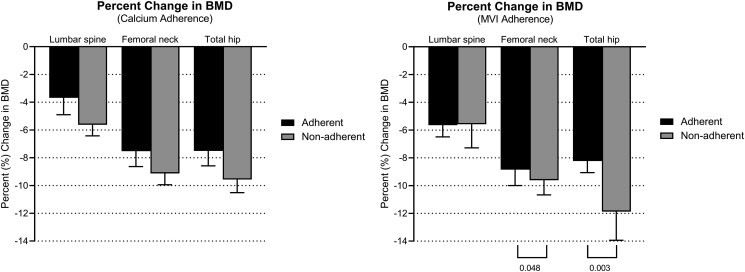
Results: Almost all patients (92/94, 98%) lost a substantial amount of weight post-TG, with an average weight loss of 26.5% at 12 months post-surgery. Serum biomarkers of mineral metabolism, namely calcium and phosphorus, did not change significantly after TG. However, average BMD was decreased in all patients at 12 months post-TG. Nonadherence to calcium supplementation was associated with a decrease in BMD. Nonadherence to multivitamin supplementation was associated with greater percent BMD loss in the femoral neck and total hip.
Conclusions: Appropriate micronutrient supplementation and nutritional counseling pre- and postoperatively in patients undergoing prophylactic TG are important to mitigate the long-term effects of gastrectomy on bone health.
Trial registration: ClinicalTrials.gov NCT03030404.
Keywords: bone health; micronutrient supplementation; prophylactic total gastrectomy.
Published by Oxford University Press on behalf of the Endocrine Society 2023.
Figures
References
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
