

Chemotherapy response in low-grade serous ovarian carcinoma at a comprehensive cancer center: Readdressing the roles of platinum and cytotoxic therapies
- PMID: 36951509
- PMCID: PMC10682957
- DOI: 10.1002/cncr.34753
Chemotherapy response in low-grade serous ovarian carcinoma at a comprehensive cancer center: Readdressing the roles of platinum and cytotoxic therapies
Abstract
Background: Data on platinum sensitivity of low-grade serous ovarian carcinoma (LGSOC) in the upfront setting is lacking, and there is limited and contradictory information on chemotherapy responses in recurrent disease.
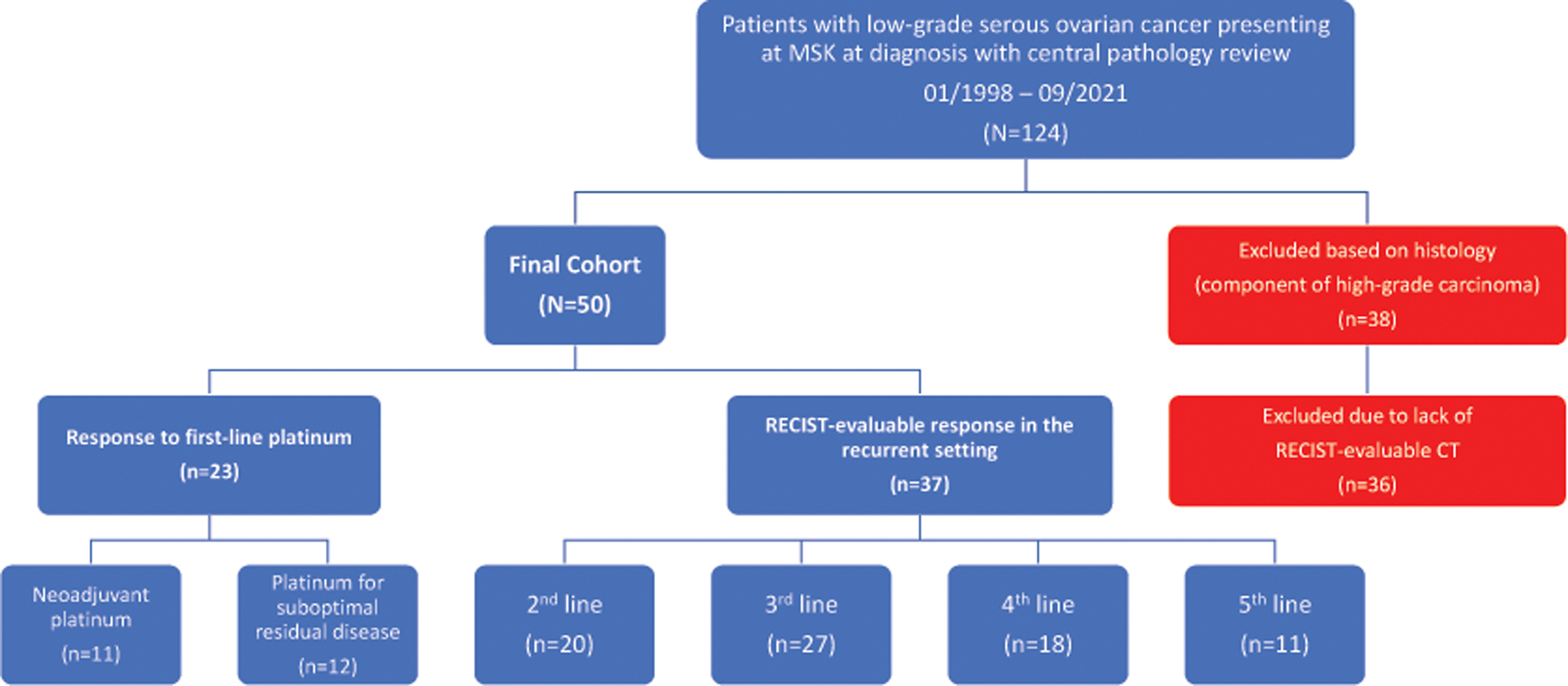
Methods: Patients with LGSOC seen at a comprehensive cancer center from January 1, 1998 to September 30, 2021 were identified from institutional databases. Response to neoadjuvant chemotherapy (NACT) or adjuvant platinum-based chemotherapy and to second- to fifth-line regimens was retrospectively characterized by Response Evaluation Criteria in Solid Tumors (RECIST) v1.1. Wilcoxon rank-sum and two-tailed Fisher exact tests were employed.
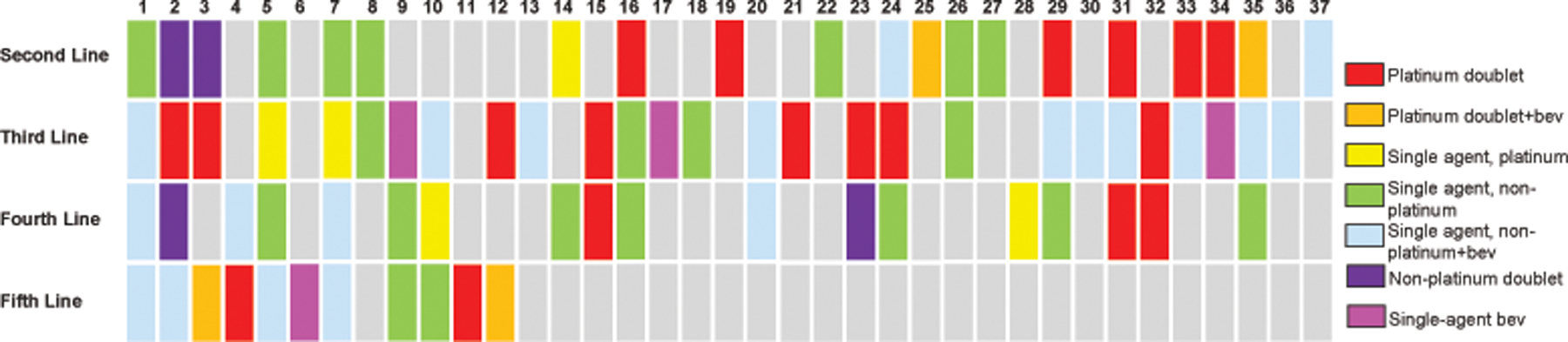
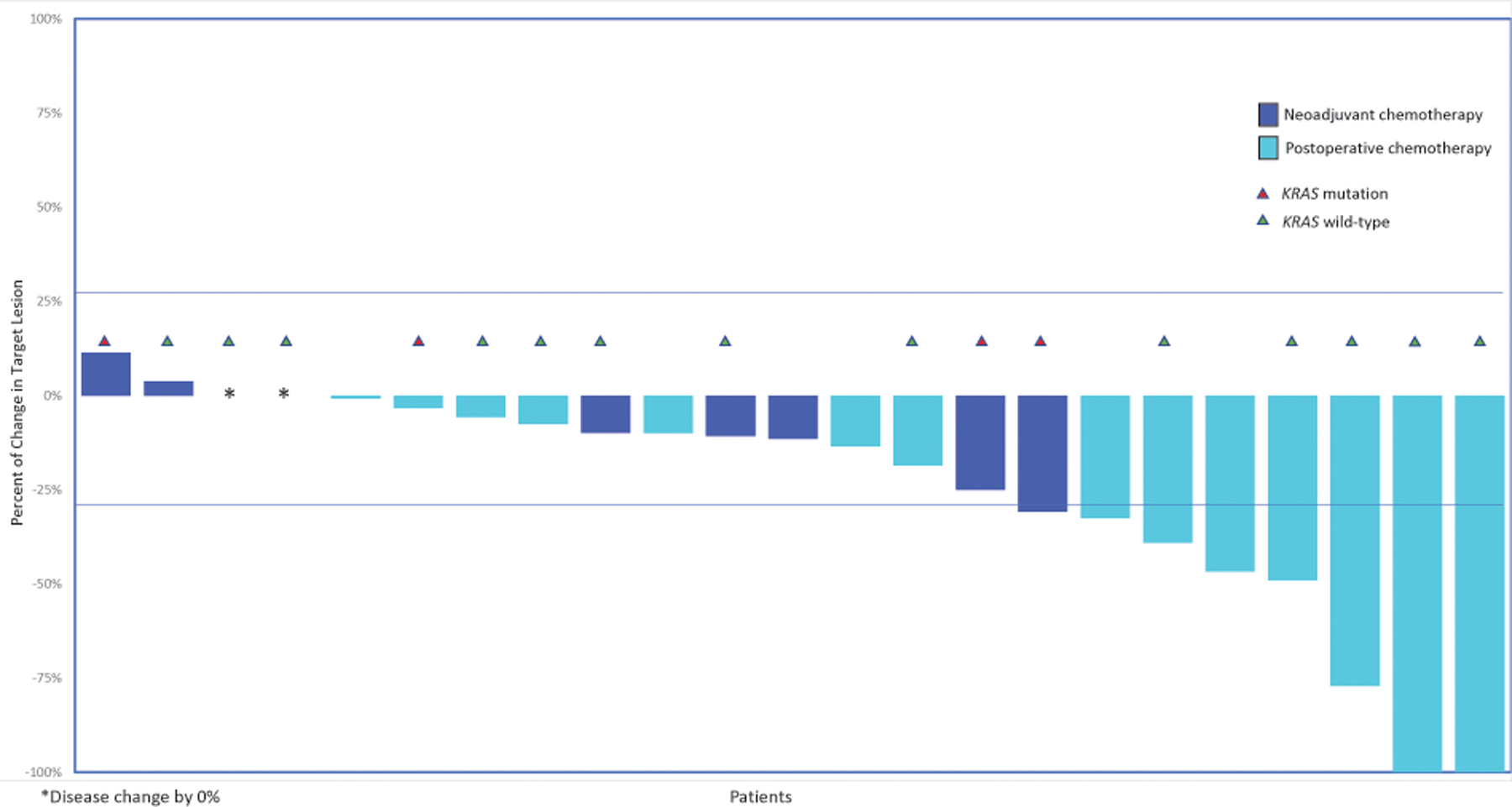
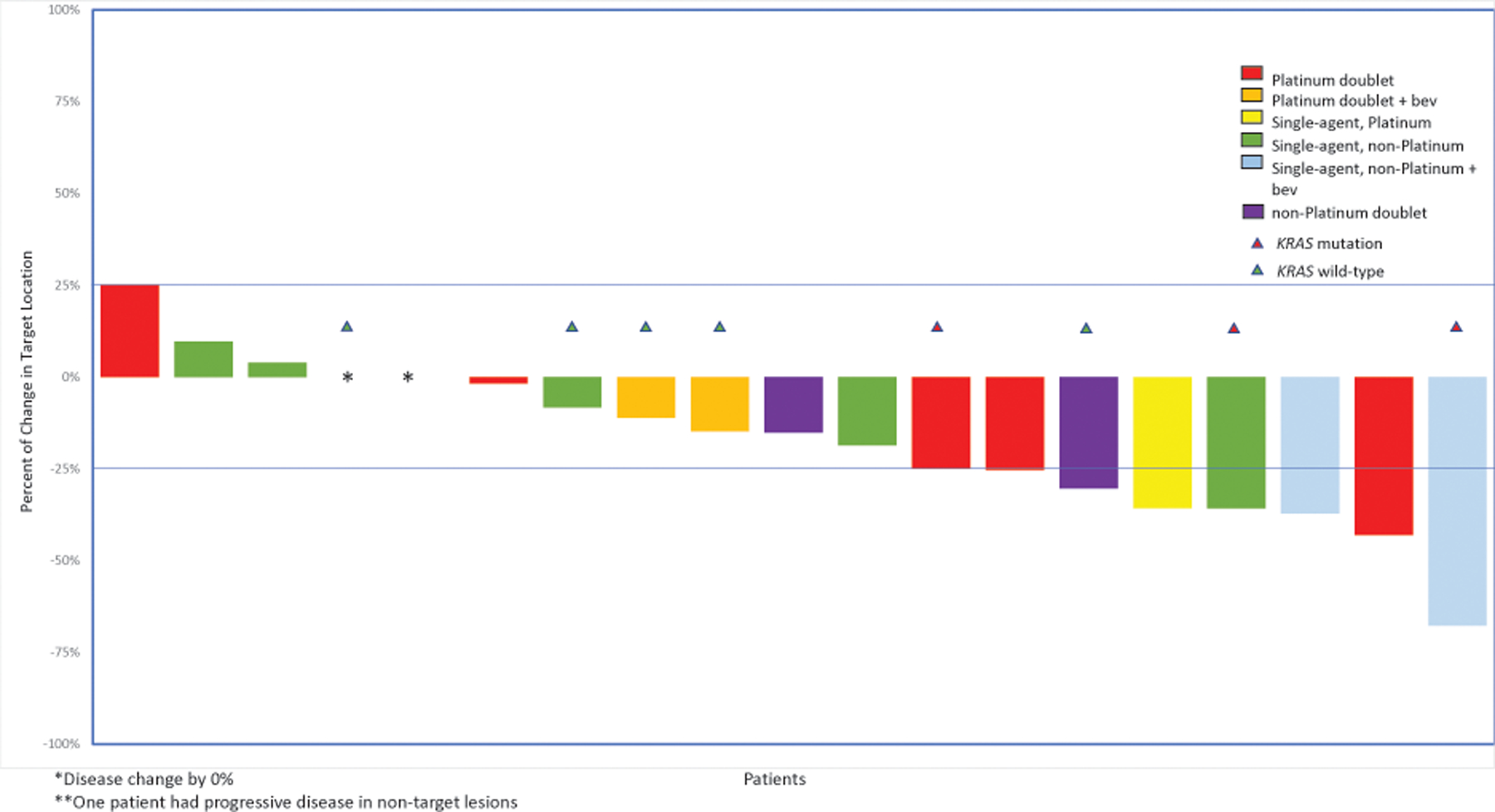
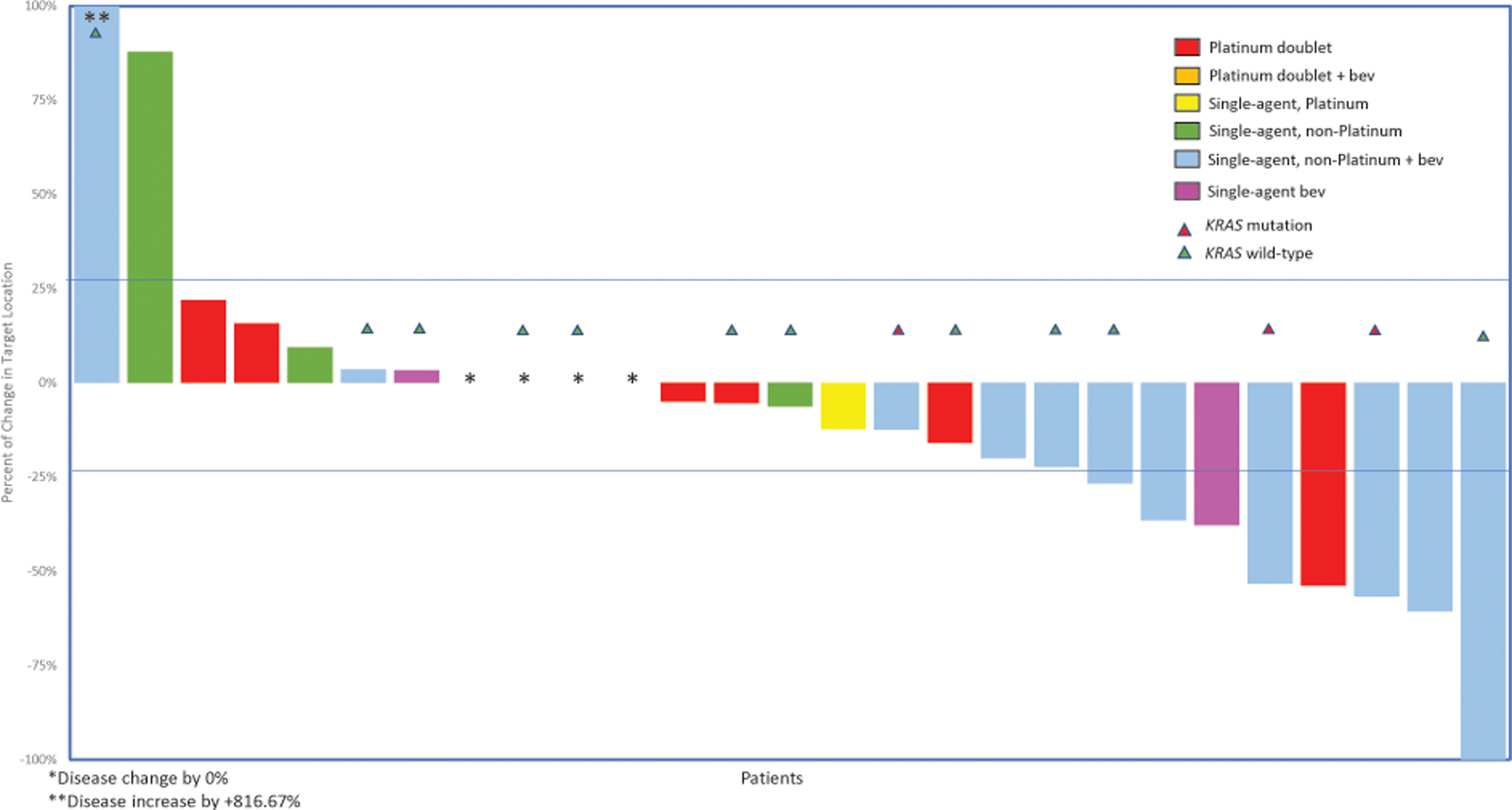
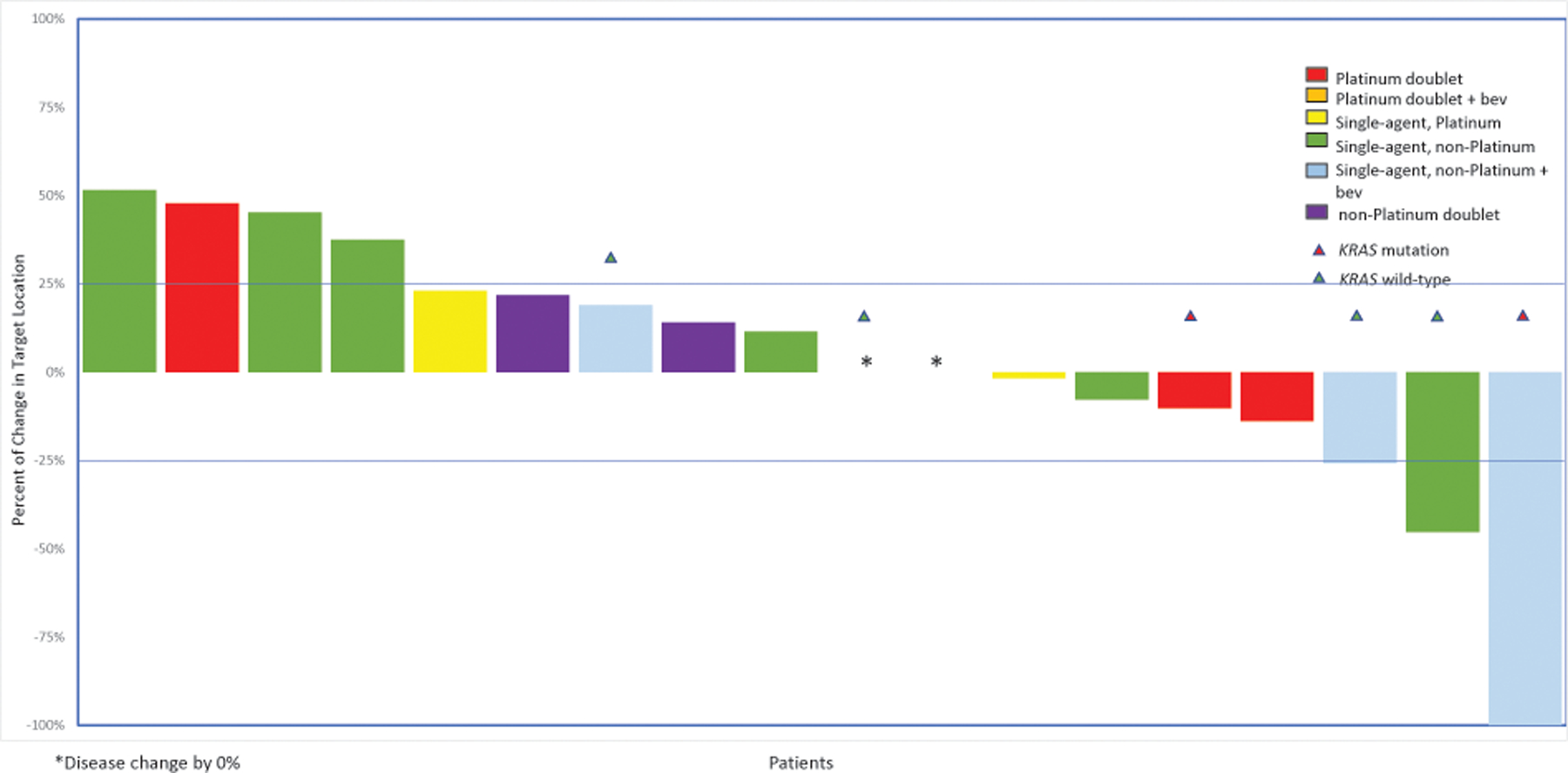
Results: Of 50 patients, 12 received platinum doublets for suboptimal residual disease and 11 as NACT. Of 12 patients with suboptimal residual disease, seven (58%) achieved objective responses (five partial responses [PRs] and two complete responses); of the 11 patients who underwent NACT, one (9%) achieved a PR (p = .027). The 15 remaining patients had stable disease on first-line platinum chemotherapy. Of 44 patients who recurred, 20 had RECIST-evaluable responses to second-line and 27 to third-line chemotherapy. Objective response rates to platinum-based chemotherapy were 22% (two of nine) in the second line and 10% (one of 10) in the third. In second and third lines, highest response rates were observed with nonplatinum chemotherapy with bevacizumab, at 100% (two of two) and 30% (three of 10), respectively.
Conclusions: Primary platinum-based chemotherapy has moderate activity in LGSOC and minimal activity in the recurrent setting, suggesting standard definitions of platinum sensitivity may not apply in LGSOC. In the second and third lines, nonplatinum chemotherapy/bevacizumab elicited the highest response rates.
Keywords: KRAS; chemotherapy; cytoreduction surgical procedures; low-grade serous ovarian cancer; neoadjuvant.
© 2023 American Cancer Society.
Conflict of interest statement
Figures
Similar articles
-
Recurrent low-grade serous ovarian carcinoma is relatively chemoresistant.Gynecol Oncol. 2009 Jul;114(1):48-52. doi: 10.1016/j.ygyno.2009.03.001. Epub 2009 Apr 10. Gynecol Oncol. 2009. PMID: 19361839
-
The role of neoadjuvant chemotherapy in the management of low-grade serous carcinoma of the ovary and peritoneum: Further evidence of relative chemoresistance.Gynecol Oncol. 2020 Sep;158(3):653-658. doi: 10.1016/j.ygyno.2020.06.498. Epub 2020 Jul 22. Gynecol Oncol. 2020. PMID: 32709538
-
Bevacizumab combined with chemotherapy in the treatment of recurrence or platinum-refractory ovarian cancer: a retrospective study of 37 cases.Indian J Cancer. 2014 Mar;51 Suppl 3:e92-4. doi: 10.4103/0019-509X.154079. Indian J Cancer. 2014. PMID: 25818742
-
Advances in precision therapy of low-grade serous ovarian cancer: A review.Medicine (Baltimore). 2024 Apr 26;103(17):e34306. doi: 10.1097/MD.0000000000034306. Medicine (Baltimore). 2024. PMID: 38669365 Free PMC article. Review.
-
Low-Grade Serous Ovarian Cancer: Current Treatment Paradigms and Future Directions.Curr Treat Options Oncol. 2018 Sep 18;19(11):54. doi: 10.1007/s11864-018-0571-8. Curr Treat Options Oncol. 2018. PMID: 30225651 Review.
Cited by
-
Primary Low-Grade Peritoneal Serous Carcinoma in a Woman With Psammoma Bodies on Cervicovaginal Cytology.Cureus. 2024 May 25;16(5):e61056. doi: 10.7759/cureus.61056. eCollection 2024 May. Cureus. 2024. PMID: 38916020 Free PMC article.
-
Folate receptor alpha expression in low-grade serous ovarian cancer: Exploring new therapeutic possibilities.Gynecol Oncol. 2024 Sep;188:52-57. doi: 10.1016/j.ygyno.2024.06.008. Epub 2024 Jun 27. Gynecol Oncol. 2024. PMID: 38941962
-
Exploring novel approaches in the systemic therapy of low-grade serous carcinoma of the ovary: a literature review.Front Med (Lausanne). 2024 May 21;11:1366603. doi: 10.3389/fmed.2024.1366603. eCollection 2024. Front Med (Lausanne). 2024. PMID: 38835797 Free PMC article. Review.
-
The highs and lows of serous ovarian cancer.Cancer. 2023 Sep 1;129(17):2613-2620. doi: 10.1002/cncr.34903. Epub 2023 Jun 27. Cancer. 2023. PMID: 37366225 Free PMC article. Review.
-
Molecular changes driving low-grade serous ovarian cancer and implications for treatment.Int J Gynecol Cancer. 2024 Oct 7;34(10):1630-1638. doi: 10.1136/ijgc-2024-005305. Int J Gynecol Cancer. 2024. PMID: 38950921 Free PMC article. Review.
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
