

Longitudinal biomarkers and kidney disease progression after acute kidney injury
- PMID: 36951957
- PMCID: PMC10243801
- DOI: 10.1172/jci.insight.167731
Longitudinal biomarkers and kidney disease progression after acute kidney injury
Abstract
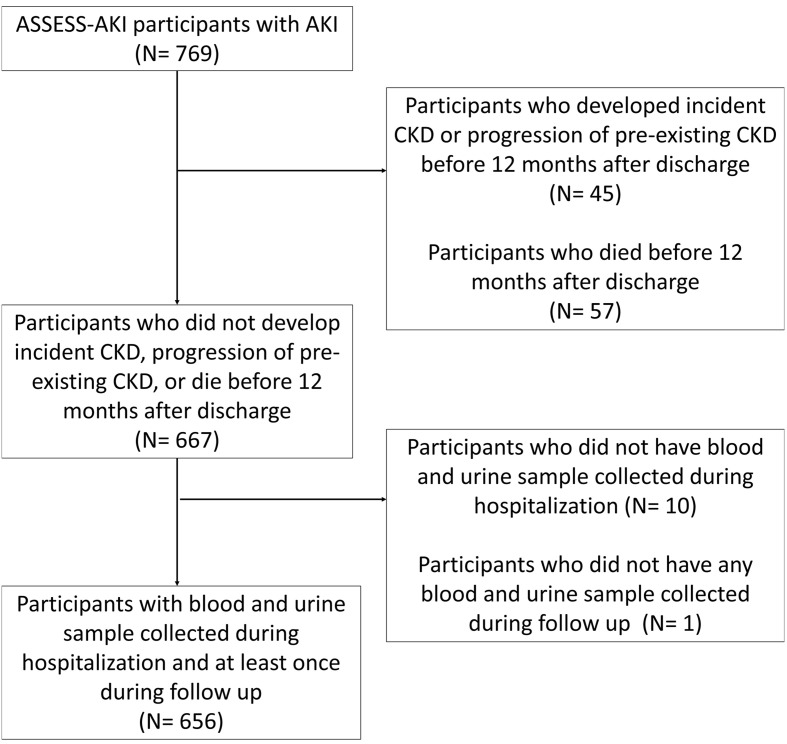
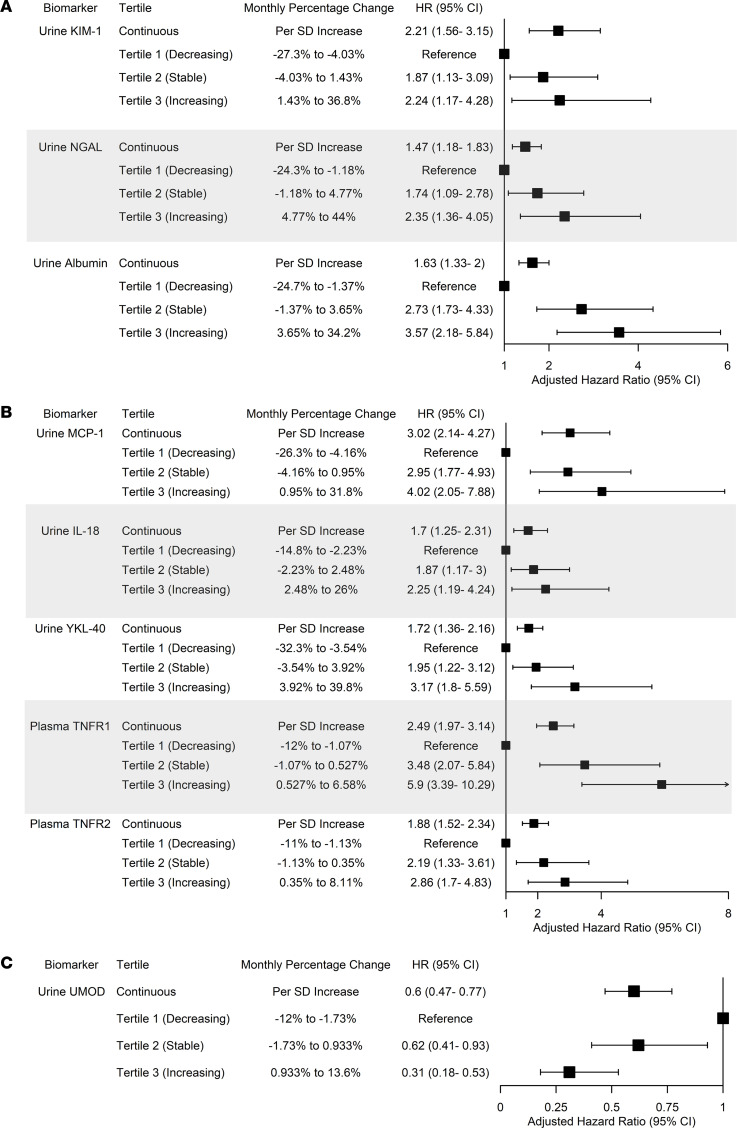
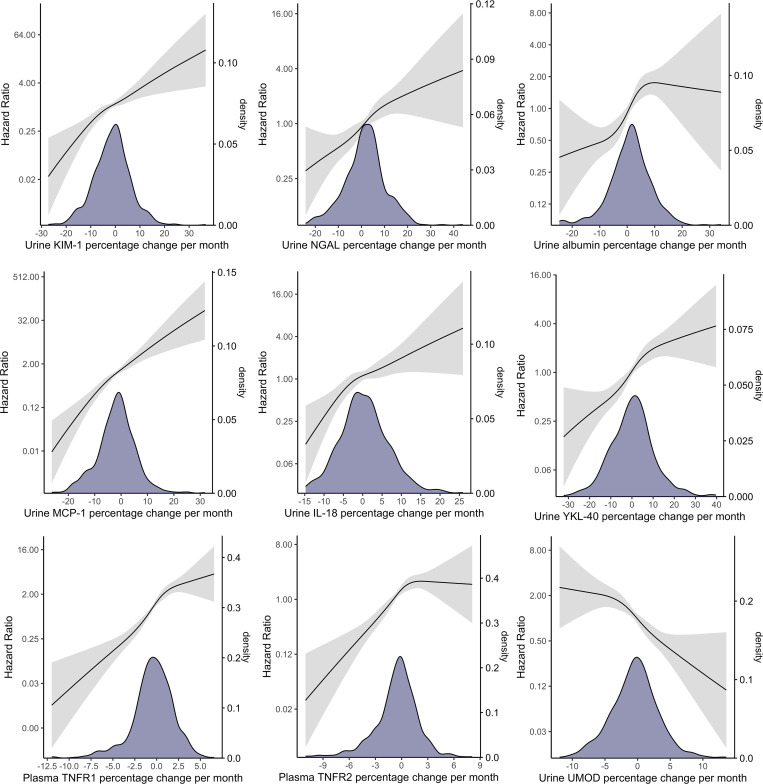
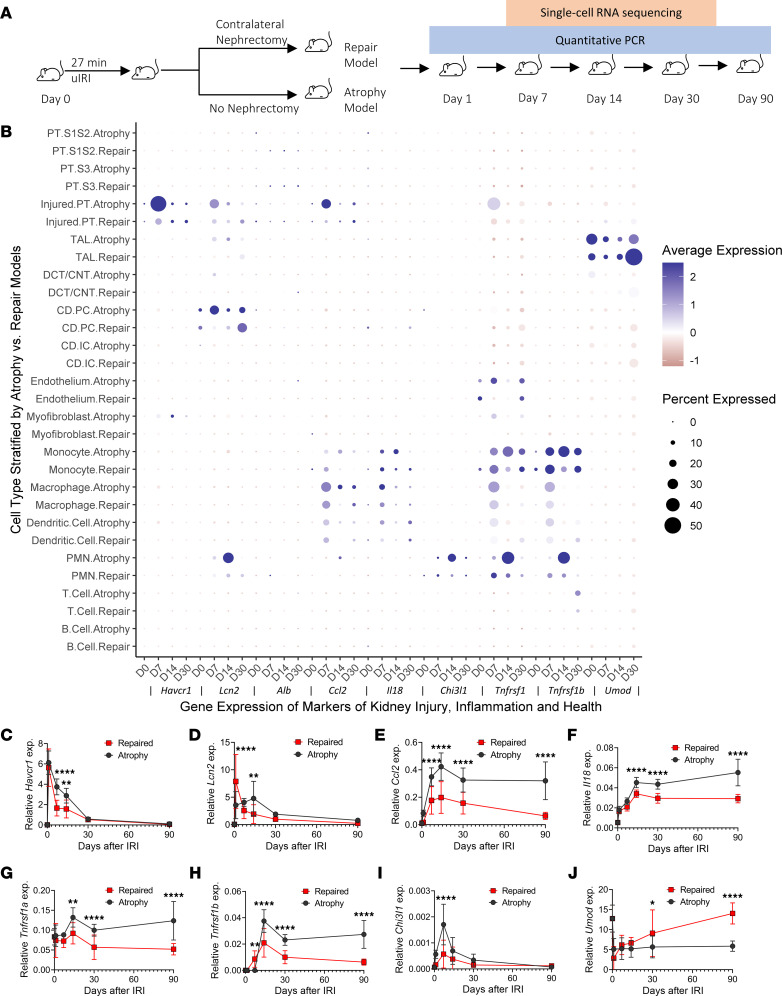
BACKGROUNDLongitudinal investigations of murine acute kidney injury (AKI) suggest that injury and inflammation may persist long after the initial insult. However, the evolution of these processes and their prognostic values are unknown in patients with AKI.METHODSIn a prospective cohort of 656 participants hospitalized with AKI, we measured 7 urine and 2 plasma biomarkers of kidney injury, inflammation, and tubular health at multiple time points from the diagnosis to 12 months after AKI. We used linear mixed-effect models to estimate biomarker changes over time, and we used Cox proportional hazard regressions to determine their associations with a composite outcome of chronic kidney disease (CKD) incidence and progression. We compared the gene expression kinetics of biomarkers in murine models of repair and atrophy after ischemic reperfusion injury (IRI).RESULTSAfter 4.3 years, 106 and 52 participants developed incident CKD and CKD progression, respectively. Each SD increase in the change of urine KIM-1, MCP-1, and plasma TNFR1 from baseline to 12 months was associated with 2- to 3-fold increased risk for CKD, while the increase in urine uromodulin was associated with 40% reduced risk for CKD. The trajectories of these biological processes were associated with progression to kidney atrophy in mice after IRI.CONCLUSIONSustained tissue injury and inflammation, and slower restoration of tubular health, are associated with higher risk of kidney disease progression. Further investigation into these ongoing biological processes may help researchers understand and prevent the AKI-to-CKD transition.FUNDINGNIH and NIDDK (grants U01DK082223, U01DK082185, U01DK082192, U01DK082183, R01DK098233, R01DK101507, R01DK114014, K23DK100468, R03DK111881, K01DK120783, and R01DK093771).
Keywords: Chronic kidney disease; Diagnostics; Epidemiology; Nephrology.
Conflict of interest statement
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
- R01 HL085757/HL/NHLBI NIH HHS/United States
- R01 DK093770/DK/NIDDK NIH HHS/United States
- R01 DK114014/DK/NIDDK NIH HHS/United States
- U01 DK082185/DK/NIDDK NIH HHS/United States
- K01 DK120783/DK/NIDDK NIH HHS/United States
- K23 DK117065/DK/NIDDK NIH HHS/United States
- R01 DK128087/DK/NIDDK NIH HHS/United States
- UL1 TR001863/TR/NCATS NIH HHS/United States
- U01 DK082183/DK/NIDDK NIH HHS/United States
- R01 DK093771/DK/NIDDK NIH HHS/United States
- R01 DK101507/DK/NIDDK NIH HHS/United States
- R01 DK098233/DK/NIDDK NIH HHS/United States
- R03 DK111881/DK/NIDDK NIH HHS/United States
- U01 DK082192/DK/NIDDK NIH HHS/United States
- UH3 DK114866/DK/NIDDK NIH HHS/United States
- U01 DK082223/DK/NIDDK NIH HHS/United States
- K23 DK100468/DK/NIDDK NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
Miscellaneous
