

Five years of experience in the Epigenetics and Chromatin Clinic: what have we learned and where do we go from here?
- PMID: 36952035
- PMCID: PMC10034257
- DOI: 10.1007/s00439-023-02537-1
Five years of experience in the Epigenetics and Chromatin Clinic: what have we learned and where do we go from here?
Abstract
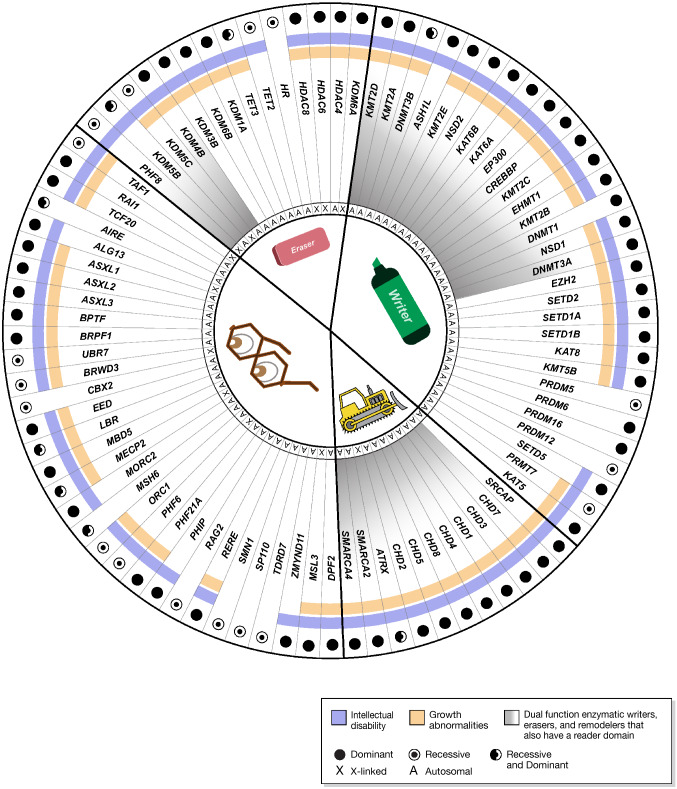
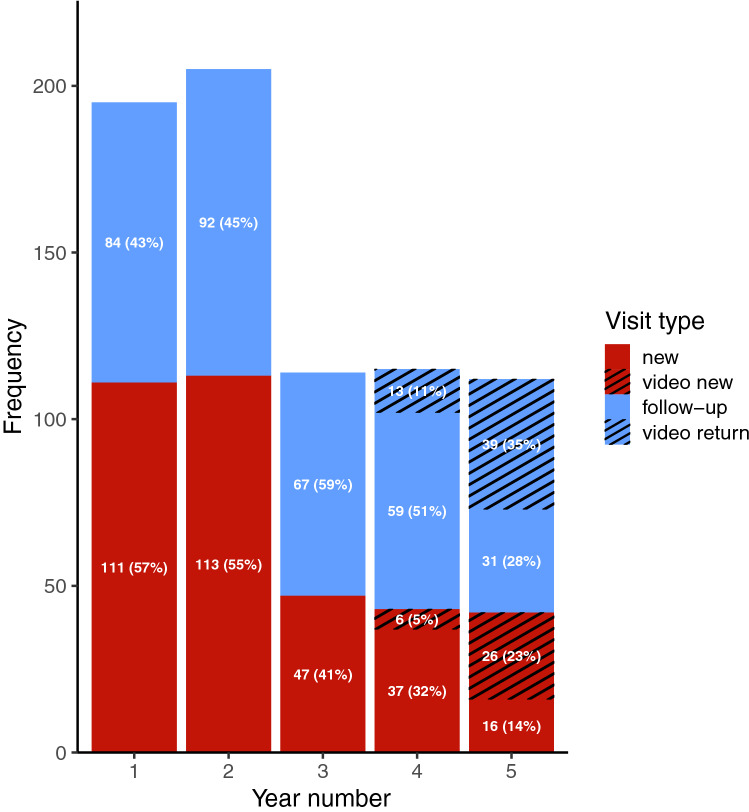
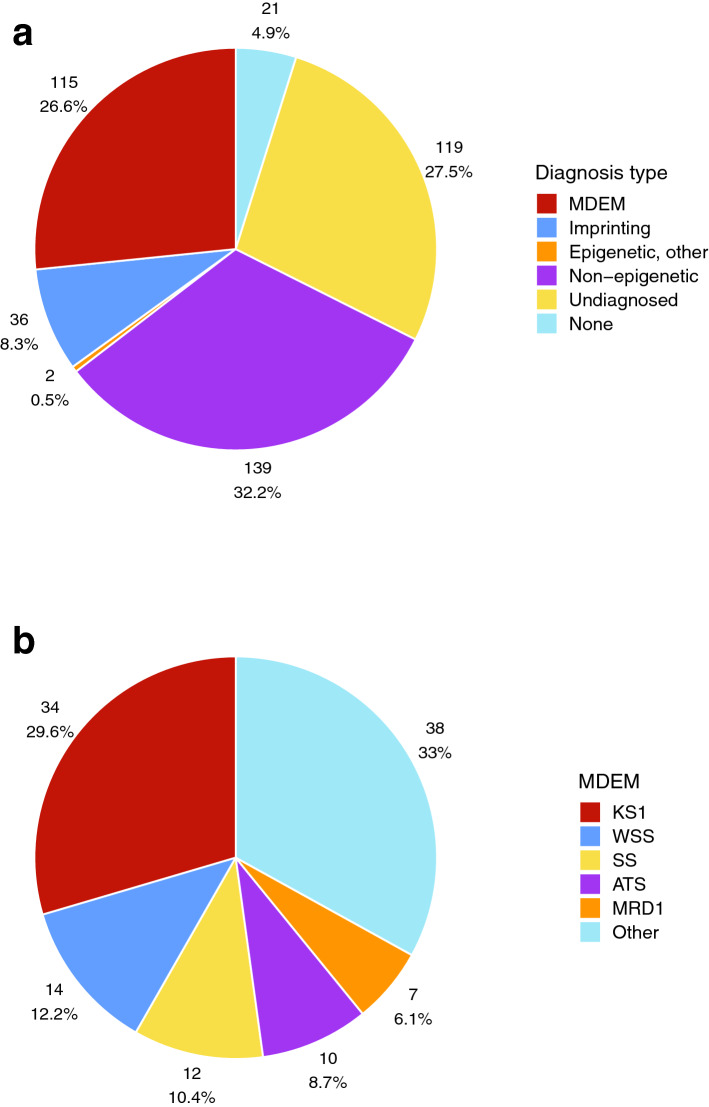
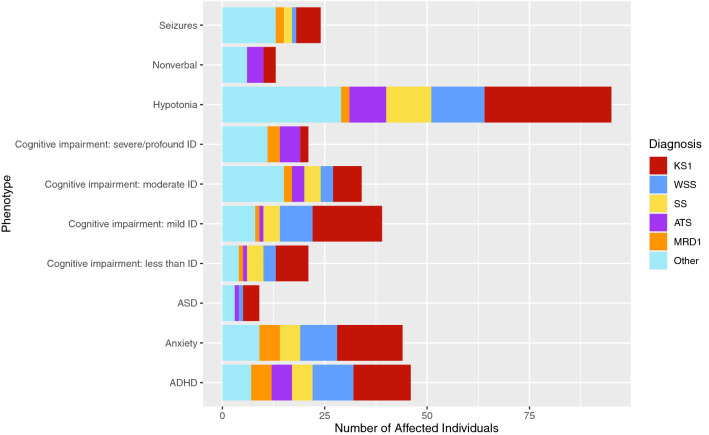
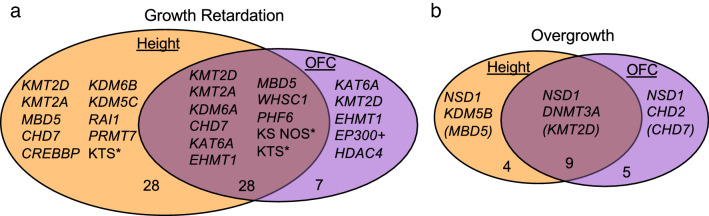
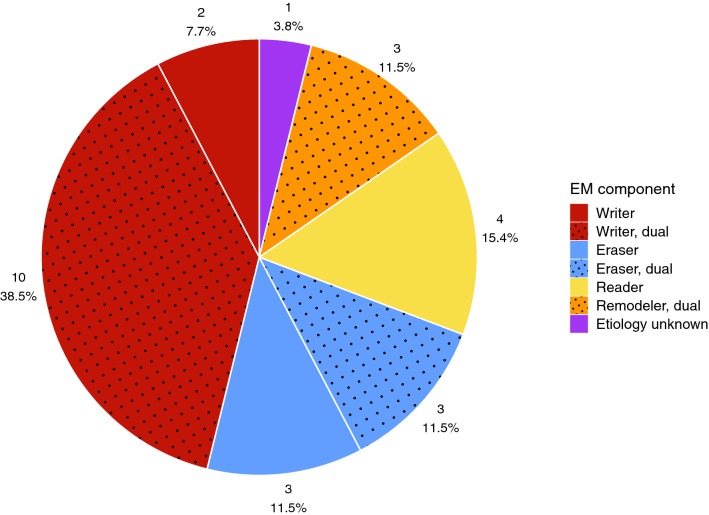
The multidisciplinary Epigenetics and Chromatin Clinic at Johns Hopkins provides comprehensive medical care for individuals with rare disorders that involve disrupted epigenetics. Initially centered on classical imprinting disorders, the focus shifted to the rapidly emerging group of genetic disorders resulting from pathogenic germline variants in epigenetic machinery genes. These are collectively called the Mendelian disorders of the epigenetic machinery (MDEMs), or more broadly, Chromatinopathies. In five years, 741 clinic visits have been completed for 432 individual patients, with 153 having confirmed epigenetic diagnoses. Of these, 115 individuals have one of 26 MDEMs with every single one exhibiting global developmental delay and/or intellectual disability. This supports prior observations that intellectual disability is the most common phenotypic feature of MDEMs. Additional common phenotypes in our clinic include growth abnormalities and neurodevelopmental issues, particularly hypotonia, attention-deficit/hyperactivity disorder (ADHD), and anxiety, with seizures and autism being less common. Overall, our patient population is representative of the broader group of MDEMs and includes mostly autosomal dominant disorders impacting writers more so than erasers, readers, and remodelers of chromatin marks. There is an increased representation of dual function components with a reader and an enzymatic domain. As expected, diagnoses were made mostly by sequencing but were aided in some cases by DNA methylation profiling. Our clinic has helped to facilitate the discovery of two new disorders, and our providers are actively developing and implementing novel therapeutic strategies for MDEMs. These data and our high follow-up rate of over 60% suggest that we are achieving our mission to diagnose, learn from, and provide optimal care for our patients with disrupted epigenetics.
© 2023. The Author(s), under exclusive licence to Springer-Verlag GmbH Germany, part of Springer Nature.
Conflict of interest statement
HTB is a consultant for Mahzi therapeutics. JRH receives research funding from Oryzon Genomics. The other authors have no known conflicts of interest to declare.
Figures
References
-
- Alarcon JM, Malleret G, Touzani K, Vronskaya S, Ishii S, Kandel ER, Barco A. Chromatin acetylation, memory, and LTP are impaired in CBP+/- mice: a model for the cognitive deficit in Rubinstein-Taybi syndrome and its amelioration. Neuron. 2004;42(6):947–959. doi: 10.1016/j.neuron.2004.05.021. - DOI - PubMed
-
- Aref-Eshghi E, Schenkel LC, Lin H, Skinner C, Ainsworth P, Pare G, Sadikovic B. The defining DNA methylation signature of Kabuki syndrome enables functional assessment of genetic variants of unknown clinical significance. Epigenetics. 2017;12(11):923–933. doi: 10.1080/15592294.2017.1381807. - DOI - PMC - PubMed
-
- Aref-Eshghi E, Bend EG, Colaiacovo S, Caudle M, Chakrabarti R, Napier M, Sadikovic B. Diagnostic utility of genome-wide DNA methylation testing in genetically unsolved individuals with suspected hereditary conditions. Am J Hum Genet. 2019;104(4):685–700. doi: 10.1016/j.ajhg.2019.03.008. - DOI - PMC - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
