

High resolution propagation-based lung imaging at clinically relevant X-ray dose levels
- PMID: 36959233
- PMCID: PMC10036329
- DOI: 10.1038/s41598-023-30870-y
High resolution propagation-based lung imaging at clinically relevant X-ray dose levels
Abstract
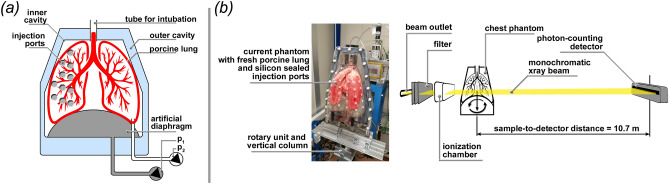
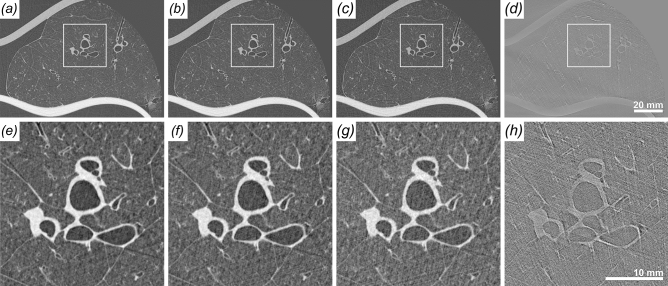
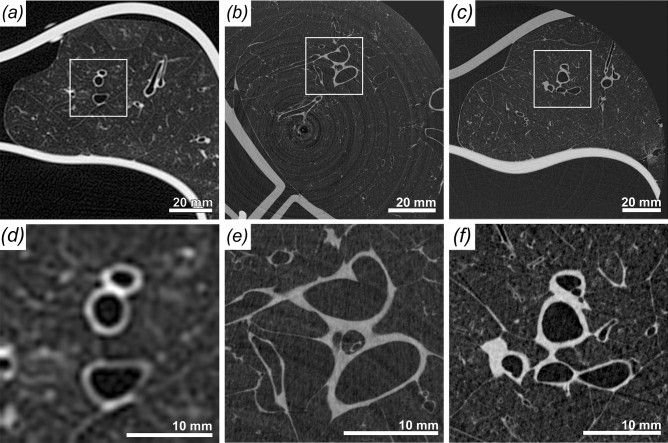
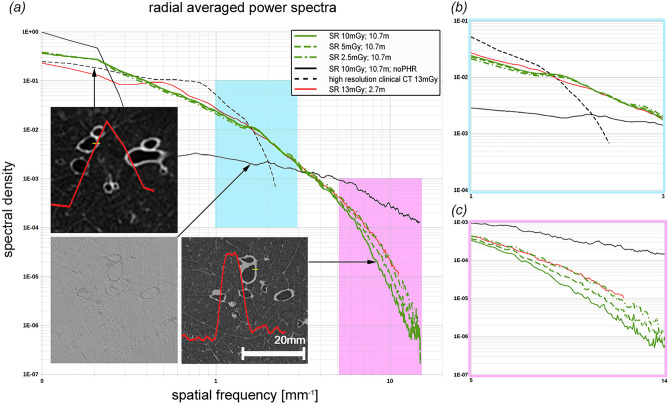
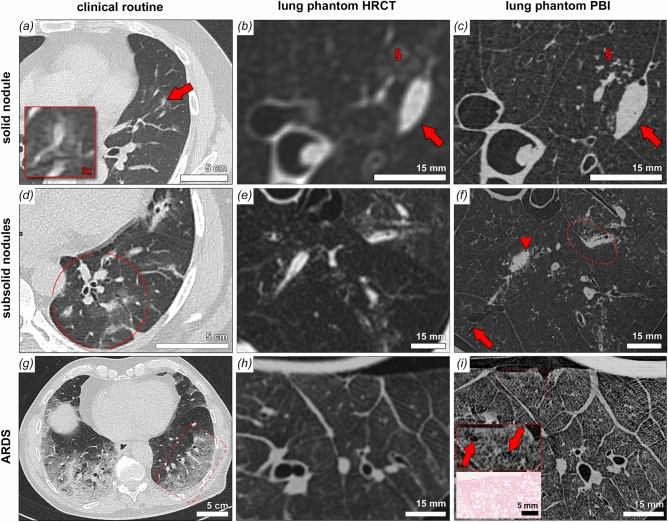
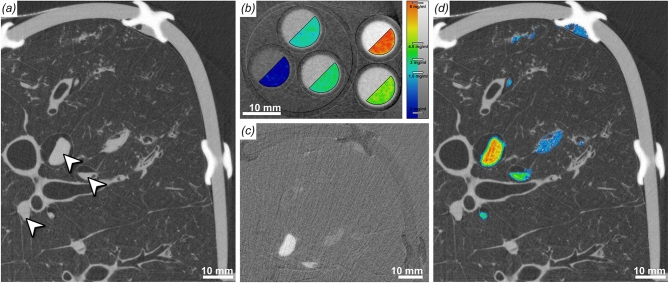
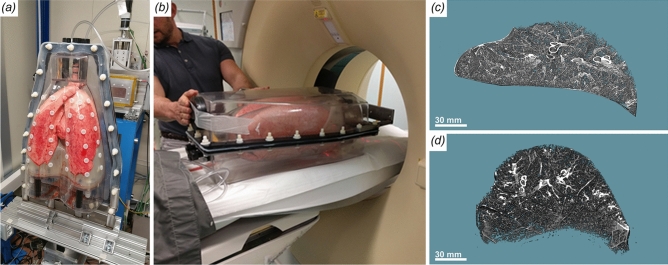
Absorption-based clinical computed tomography (CT) is the current imaging method of choice in the diagnosis of lung diseases. Many pulmonary diseases are affecting microscopic structures of the lung, such as terminal bronchi, alveolar spaces, sublobular blood vessels or the pulmonary interstitial tissue. As spatial resolution in CT is limited by the clinically acceptable applied X-ray dose, a comprehensive diagnosis of conditions such as interstitial lung disease, idiopathic pulmonary fibrosis or the characterization of small pulmonary nodules is limited and may require additional validation by invasive lung biopsies. Propagation-based imaging (PBI) is a phase sensitive X-ray imaging technique capable of reaching high spatial resolutions at relatively low applied radiation dose levels. In this publication, we present technical refinements of PBI for the characterization of different artificial lung pathologies, mimicking clinically relevant patterns in ventilated fresh porcine lungs in a human-scale chest phantom. The combination of a very large propagation distance of 10.7 m and a photon counting detector with [Formula: see text] pixel size enabled high resolution PBI CT with significantly improved dose efficiency, measured by thermoluminescence detectors. Image quality was directly compared with state-of-the-art clinical CT. PBI with increased propagation distance was found to provide improved image quality at the same or even lower X-ray dose levels than clinical CT. By combining PBI with iodine k-edge subtraction imaging we further demonstrate that, the high quality of the calculated iodine concentration maps might be a potential tool for the analysis of lung perfusion in great detail. Our results indicate PBI to be of great value for accurate diagnosis of lung disease in patients as it allows to depict pathological lesions non-invasively at high resolution in 3D. This will especially benefit patients at high risk of complications from invasive lung biopsies such as in the setting of suspected idiopathic pulmonary fibrosis (IPF).
© 2023. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- Kalender, W. A. Computed tomography: fundamentals, system technology, image quality, applications (John Wiley & Sons, 2011).
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
