

Smartphone-assisted training with education for patients with hip and/or knee osteoarthritis (SmArt-E): study protocol for a multicentre pragmatic randomized controlled trial
- PMID: 36959595
- PMCID: PMC10034894
- DOI: 10.1186/s12891-023-06255-7
Smartphone-assisted training with education for patients with hip and/or knee osteoarthritis (SmArt-E): study protocol for a multicentre pragmatic randomized controlled trial
Abstract
Introduction: Hip and knee osteoarthritis are associated with functional limitations, pain and restrictions in quality of life and the ability to work. Furthermore, with growing prevalence, osteoarthritis is increasingly causing (in)direct costs. Guidelines recommend exercise therapy and education as primary treatment strategies. Available options for treatment based on physical activity promotion and lifestyle change are often insufficiently provided and used. In addition, the quality of current exercise programmes often does not meet the changing care needs of older people with comorbidities and exercise adherence is a challenge beyond personal physiotherapy. The main objective of this study is to investigate the short- and long-term (cost-)effectiveness of the SmArt-E programme in people with hip and/or knee osteoarthritis in terms of pain and physical functioning compared to usual care.
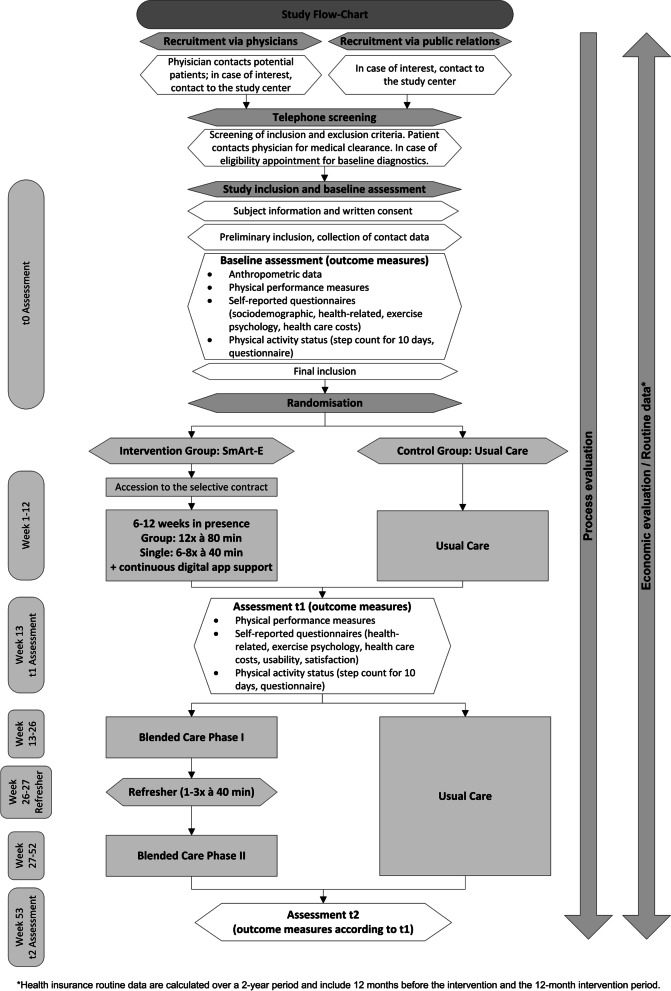
Methods: This study is designed as a multicentre randomized controlled trial with a target sample size of 330 patients. The intervention is based on the e-Exercise intervention from the Netherlands, consists of a training and education programme and is conducted as a blended care intervention over 12 months. We use an app to support independent training and the development of self-management skills. The primary and secondary hypotheses are that participants in the SmArt-E intervention will have less pain (numerical rating scale) and better physical functioning (Hip Disability and Osteoarthritis Outcome Score, Knee Injury and Osteoarthritis Outcome Score) compared to participants in the usual care group after 12 and 3 months. Other secondary outcomes are based on domains of the Osteoarthritis Research Society International (OARSI). The study will be accompanied by a process evaluation.
Discussion: After a positive evaluation, SmArt-E can be offered in usual care, flexibly addressing different care situations. The desired sustainability and the support of the participants' behavioural change are initiated via the app through audio-visual contact with their physiotherapists. Furthermore, the app supports the repetition and consolidation of learned training and educational content. For people with osteoarthritis, the new form of care with proven effectiveness can lead to a reduction in underuse and misuse of care as well as contribute to a reduction in (in)direct costs.
Trial registration: German Clinical Trials Register, DRKS00028477. Registered on August 10, 2022.
Keywords: Combined modality therapy; Education; Exercise therapy; Osteoarthritis; Physical therapy modalities; Telerehabilitation.
© 2023. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures




References
-
- Postler A, Ramos AL, Goronzy J, Günther K-P, Lange T, Schmitt J, et al. Prevalence and treatment of hip and knee osteoarthritis in people aged 60 years or older in Germany: an analysis based on health insurance claims data. Clin Interv Aging. 2018;13:2339–2349. doi: 10.2147/CIA.S174741. - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
