

Simulation-based training for embryo transfer for clinicians with differing levels of expertise: an application of the American Society for Reproductive Medicine Embryo Transfer Simulator
- PMID: 36959969
- PMCID: PMC10028427
- DOI: 10.1016/j.xfre.2022.08.003
Simulation-based training for embryo transfer for clinicians with differing levels of expertise: an application of the American Society for Reproductive Medicine Embryo Transfer Simulator
Abstract
Objective: To compare the learning curve of clinicians with different levels of embryo transfer (ET) experience using the American Society for Reproductive Medicine (ASRM) Embryo Transfer Simulator.
Design: Prospective cohort study.
Setting: Single large university-affiliated in vitro fertilization center.
Patients: Participants with 3 levels of expertise with ET were recruited: "group 1" (Reproductive Endocrinology and Infertility attendings), "group 2" (Reproductive Endocrinology and Infertility nurses, advance practice providers, or medical assistants), and "group 3" (Obstetrics and Gynecology resident physicians).
Interventions: All participants completed ET simulation training using uterine cases A, B, and C (easiest to most difficult) of the ASRM ET Simulator. Participants completed each case 5 times for a total of 15 repetitions.
Main outcome measures: The primary outcome was ET simulation scores analyzed at each attempt for each uterine case, with a maximum score of 155. Secondary outcomes included self-assessed comfort levels before and after the completion of the simulation and total duration of ET. Comfort was assessed using a 5-point Likert scale.
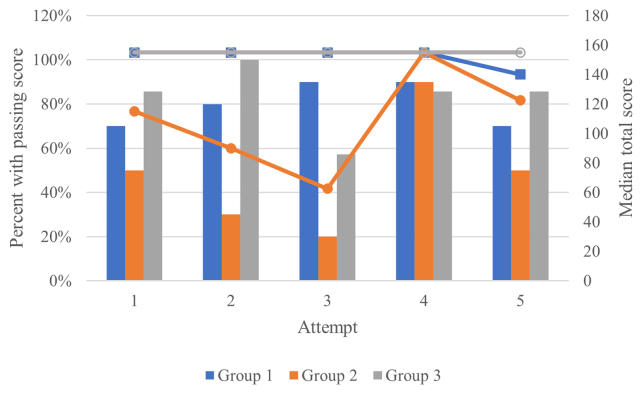
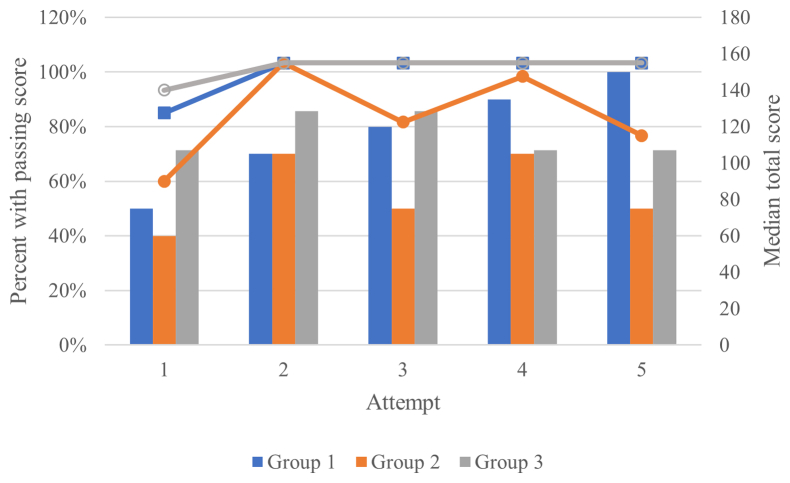
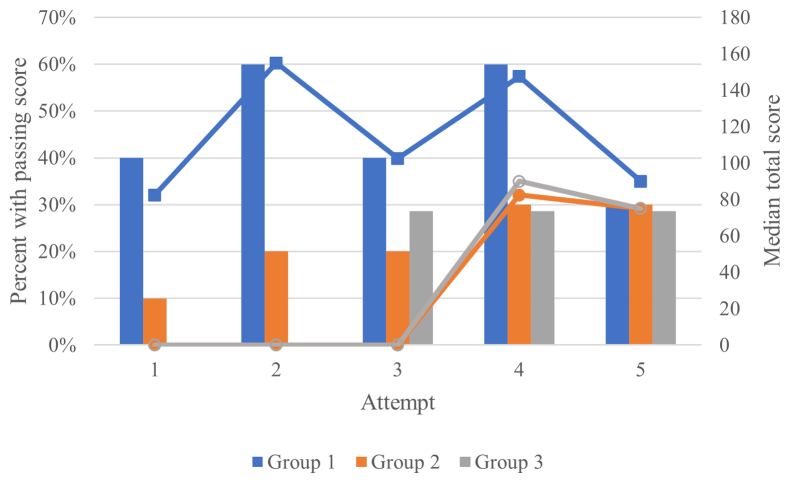
Results: Twenty-seven participants with 3 different levels of expertise with ET were recruited from December 2020 to February 2021. For cases A and B, median total scores were not significantly different between groups 1 and 3 at first or last attempts. Group 2 did not perform as well as group 3 at the beginning of case A or group 1 at the end of case B. All groups demonstrated a decrease in total time from the first attempt to the last attempt for both cases. For case C, the "difficult" uterus, groups 2 and 3 exhibited the greatest improvement in total median score: from 0 to 75 from the first to last attempt. Group 1 scored equally well from first through last attempts. Although no one from group 2 or 3 achieved a passing score with the first attempt (80% of the max score), approximately 30% had passing scores at the last attempt. Groups 1 and 3 showed a significant decrease in total time across attempts for case C. Following simulation, 100% of groups 2 and 3 reported perceived improvement in their skills. Group 3 showed significant improvement in comfort scores with Likert scores of 1.71 ± 0.76 and 1.0 ± 0.0 for the "Easy" and "Difficult" cases, respectively, before simulation and 4.57 ± 0.53 and 2.4 ± 1.1 after simulation.
Conclusions: The ASRM ET Simulator was effective in improving both technical skill and comfort level, particularly for those with little to no ET experience and was most marked when training on a difficult clinical case.
Keywords: Simulation; education; embryo transfer; training.
© 2022 The Authors.
Figures
Similar articles
-
Simulation training for embryo transfer: findings from the American Society for Reproductive Medicine Embryo Transfer Certificate Course.Fertil Steril. 2021 Apr;115(4):852-859. doi: 10.1016/j.fertnstert.2020.10.056. Epub 2020 Dec 23. Fertil Steril. 2021. PMID: 33358251
-
Embryo transfer learning using medical simulation tools: a comparison of two embryo transfer simulators.J Gynecol Obstet Hum Reprod. 2023 Mar;52(3):102542. doi: 10.1016/j.jogoh.2023.102542. Epub 2023 Jan 20. J Gynecol Obstet Hum Reprod. 2023. PMID: 36682581
-
Validation of computer simulation training for esophagogastroduodenoscopy: Pilot study.J Gastroenterol Hepatol. 2007 Aug;22(8):1214-9. doi: 10.1111/j.1440-1746.2007.04841.x. Epub 2007 Jun 7. J Gastroenterol Hepatol. 2007. PMID: 17559386
-
Guidelines for the number of embryos to transfer following in vitro fertilization No. 182, September 2006.Int J Gynaecol Obstet. 2008 Aug;102(2):203-16. doi: 10.1016/j.ijgo.2008.01.007. Int J Gynaecol Obstet. 2008. PMID: 18773532 Review.
-
Virtual reality simulation training for health professions trainees in gastrointestinal endoscopy.Cochrane Database Syst Rev. 2018 Aug 17;8(8):CD008237. doi: 10.1002/14651858.CD008237.pub3. Cochrane Database Syst Rev. 2018. PMID: 30117156 Free PMC article.
Cited by
-
The American Society for Reproductive Medicine Embryo Transfer Simulator Initiative has come full circle: an editorial.F S Rep. 2023 Jan 6;4(1):22-23. doi: 10.1016/j.xfre.2023.01.001. eCollection 2023 Mar. F S Rep. 2023. PMID: 36959961 Free PMC article. No abstract available.
References
-
- Grygoruk C., Sieczynski P., Pietrewicz P., Mrugacz M., Gagan J., Mrugacz G. Pressure changes during embryo transfer. Fertil Steril. 2011;95:538–541. - PubMed
-
- Kovacs G.T. What factors are important for successful embryo transfer after in-vitro fertilization? Hum Reprod. 1999;14:590–592. - PubMed
-
- Sallam H.N. Embryo transfer: factors involved in optimizing the success. Curr Opin Obstet Gynecol. 2005;17:289–298. - PubMed
-
- Schoolcraft W.B., Surrey E.S., Gardner D.K. Embryo transfer: techniques and variables affecting success. Fertil Steril. 2001;76:863–870. - PubMed
-
- Hearns-Stokes R.M., Miller B.T., Scott L., Creuss D., Chakraborty P.K., Segars J.H. Pregnancy rates after embryo transfer depend on the provider at embryo transfer. Fertil Steril. 2000;74:80–86. - PubMed
LinkOut - more resources
Full Text Sources
