

Neonatal and paediatric point-of-care ultrasound review
- PMID: 36960139
- PMCID: PMC10030095
- DOI: 10.1002/ajum.12322
Neonatal and paediatric point-of-care ultrasound review
Abstract
Purpose: Point-of-care ultrasound (POCUS) examinations for children and newborns are different from POCUS exams for adults due to dissimilarities in size and body composition, as well as distinct surgical procedures and pathologies in the paediatric patient. This review describes the major paediatric POCUS exams and how to perform them and summarizes the current evidence-based perioperative applications of POCUS in paediatric and neonatal patients.
Method: Literature searches using PubMed and Google Scholar databases for the period from January 2000 to November 2021 that included MeSH headings of [ultrasonography] and [point of care systems] and keywords including "ultrasound" for studies involving children aged 0 to 18 years.
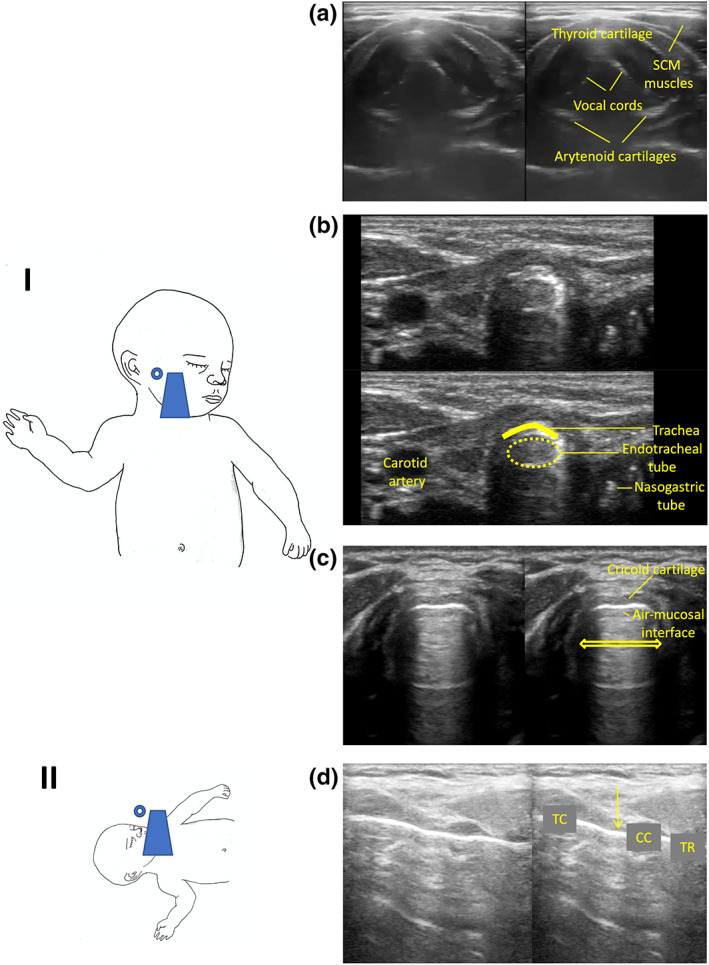
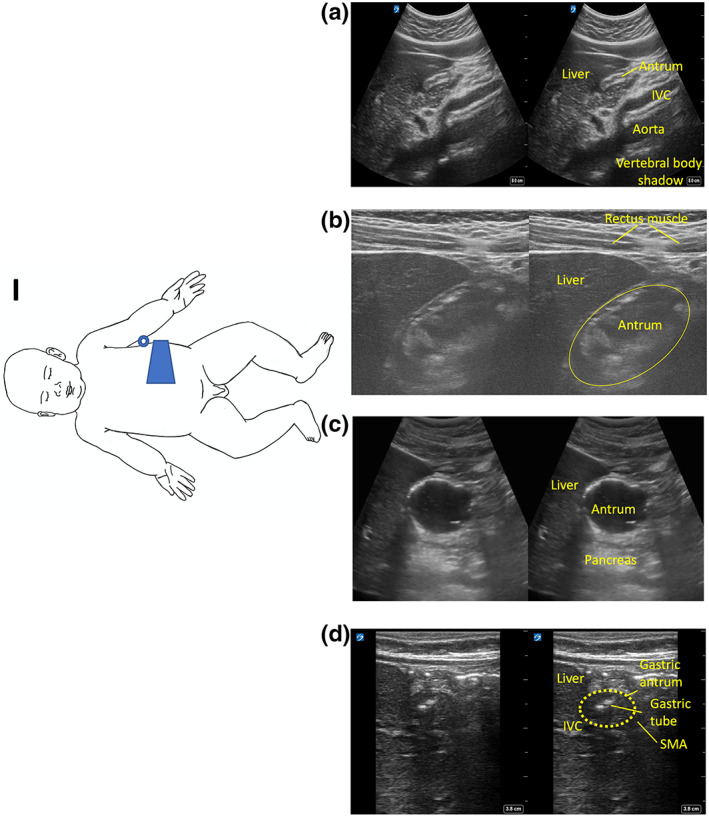
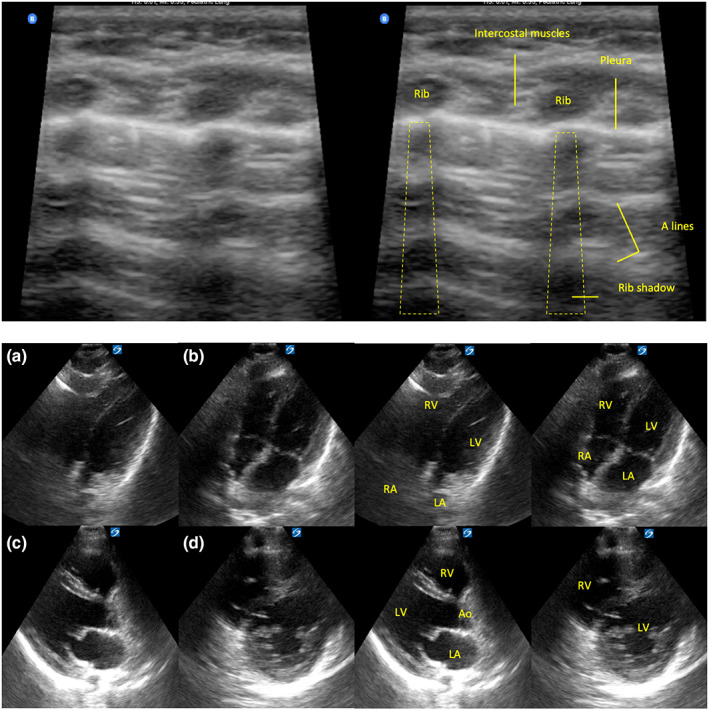
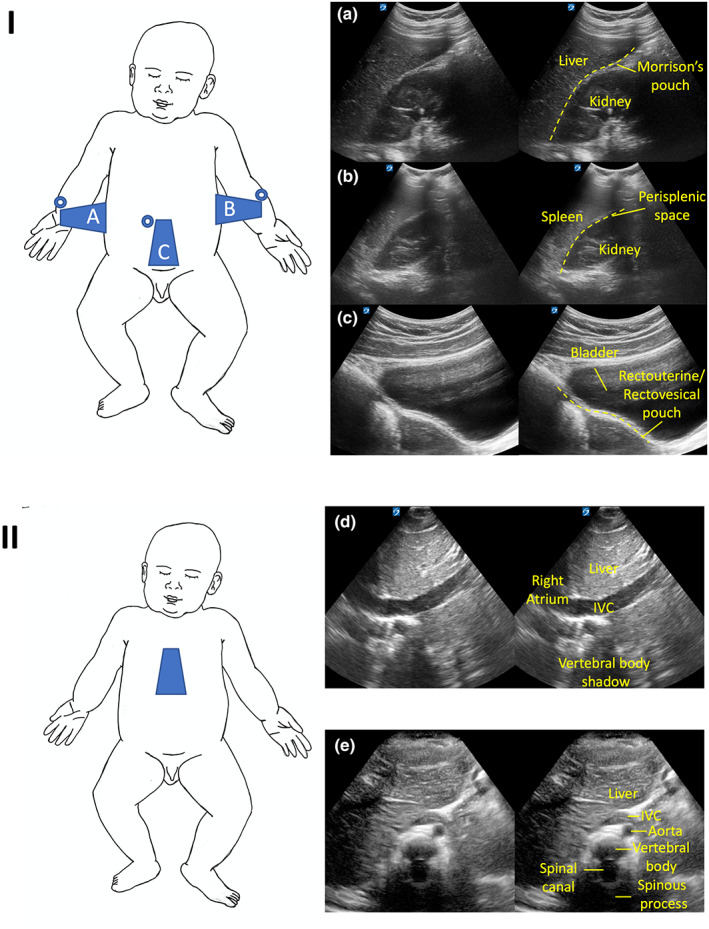
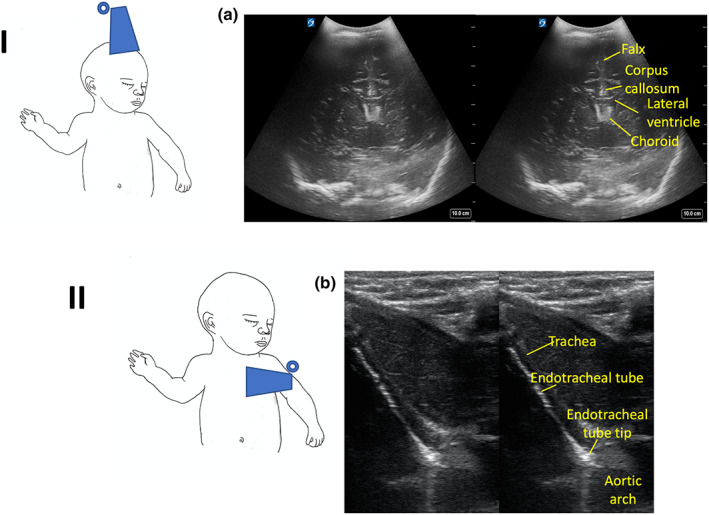
Results: Paediatric and neonatal POCUS exams can evaluate airway, gastric, pulmonary, cardiac, abdominal, vascular, and cerebral systems.
Discussion: POCUS is rapidly expanding in its utility and presence in the perioperative care of paediatric and neonatal patients as their anatomy and pathophysiology are uniquely suited for ultrasound imaging applications that extend beyond the standard adult POCUS exams.
Conclusions: Paediatric POCUS is a powerful adjunct that complements and augments clinical diagnostic evaluation and treatment.
Keywords: POCUS; children; neonate; paediatric; point‐of‐care ultrasound.
© 2022 Australasian Society for Ultrasound in Medicine.
Conflict of interest statement
None declared.
Figures
Similar articles
-
International evidence-based guidelines on Point of Care Ultrasound (POCUS) for critically ill neonates and children issued by the POCUS Working Group of the European Society of Paediatric and Neonatal Intensive Care (ESPNIC).Crit Care. 2020 Feb 24;24(1):65. doi: 10.1186/s13054-020-2787-9. Crit Care. 2020. PMID: 32093763 Free PMC article.
-
Point-of-care ultrasound in pediatric anesthesia: perioperative considerations.Curr Opin Anaesthesiol. 2020 Jun;33(3):343-353. doi: 10.1097/ACO.0000000000000852. Curr Opin Anaesthesiol. 2020. PMID: 32324662 Review.
-
Point-of-care ultrasound (POCUS) protocol for systematic assessment of the crashing neonate-expert consensus statement of the international crashing neonate working group.Eur J Pediatr. 2023 Jan;182(1):53-66. doi: 10.1007/s00431-022-04636-z. Epub 2022 Oct 14. Eur J Pediatr. 2023. PMID: 36239816 Free PMC article.
-
Feasibility Evaluation of Commercially Available Video Conferencing Devices to Technically Direct Untrained Nonmedical Personnel to Perform a Rapid Trauma Ultrasound Examination.Diagnostics (Basel). 2019 Nov 14;9(4):188. doi: 10.3390/diagnostics9040188. Diagnostics (Basel). 2019. PMID: 31739422 Free PMC article.
-
Perioperative Point of Care Ultrasound (POCUS) for Anesthesiologists: an Overview.Curr Pain Headache Rep. 2020 Mar 21;24(5):20. doi: 10.1007/s11916-020-0847-0. Curr Pain Headache Rep. 2020. PMID: 32200432 Review.
Cited by
-
Applications of Point-of-Care-Ultrasound in Neonatology: A Systematic Review of the Literature.Life (Basel). 2024 May 22;14(6):658. doi: 10.3390/life14060658. Life (Basel). 2024. PMID: 38929641 Free PMC article. Review.
References
-
- Vats A, Worley GA, de Bruyn R, Porter H, Albert DM, Bailey CM. Laryngeal ultrasound to assess vocal fold paralysis in children. J Laryngol Otol 2004; 118(6): 429–31. - PubMed
-
- Sayyid Z, Vendra V, Meister KD, Krawczeski CD, Speiser NJ, Sidell DR. Application‐based translaryngeal ultrasound for the assessment of vocal fold mobility in children. Otolaryngol Head Neck Surg 2019; 161(6): 1031–5. - PubMed
-
- Stafrace S, Engelhardt T, Teoh WH, Kristensen MS. Essential ultrasound techniques of the pediatric airway. Paediatr Anaesth 2016; 26(2): 122–31. - PubMed
-
- Mori T, Nomura O, Hagiwara Y, Inoue N. Diagnostic accuracy of a 3‐point ultrasound protocol to detect esophageal or endobronchial mainstem intubation in a pediatric emergency department. J Ultrasound Med 2019; 38(11): 2945–54. - PubMed
-
- Pillai R, Kumaran S, Jeyaseelan L, George SP, Sahajanandan R. Usefulness of ultrasound‐guided measurement of minimal transverse diameter of subglottic airway in determining the endotracheal tube size in children with congenital heart disease: a prospective observational study. Ann Card Anaesth 2018; 21(4): 382–7. - PMC - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Medical