

Review
doi: 10.1016/j.bjae.2023.01.001.
Epub 2023 Feb 22.
Infective endocarditis
Affiliations
- PMID: 36960439
- PMCID: PMC10028394
- DOI: 10.1016/j.bjae.2023.01.001
Item in Clipboard
Review
Infective endocarditis
BJA Educ.
2023 Apr.
No abstract available
Keywords: endocarditis; microbiology; valvular heart disease.
Conflict of interest statement
The authors declare that they have no conflicts of interest.
Figures
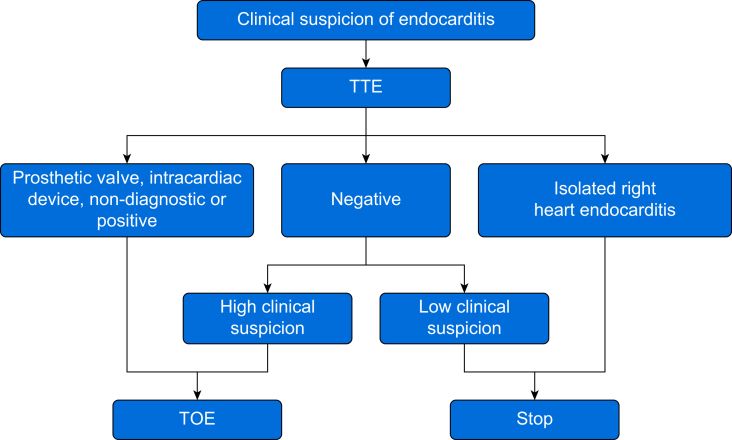
Echocardiography for suspected endocarditis. If TTE confirms isolated right heart endocarditis, proceeding to TOE may not be necessary. If the initial TOE is negative, but high suspicion remains, a repeat examination may be required within 5–7 days.

(A) Transoesophageal echocardiographic view of the left ventricular outflow tract in the mid-oesophageal long-axis view. A small, rounded, smooth mass is seen adherent to the right coronary cusp of the aortic valve. Colour Doppler imaging demonstrated no valvular stenosis or regurgitation. The smooth appearance and position of the mass indicate this mass as a likely fibroelastoma rather than vegetation. (B) The same view with zoom function enabled. In this case, TOE was useful to help exclude the diagnosis of endocarditis. AV, aortic valve; LA, left atrium; LV, left ventricle; LVOT, left ventricular outflow tract; MV, mitral valve. (If reading the pdf online, click on the image to view the video.)

Transthoracic echocardiographic apical four-chamber view showing a highly abnormal mitral valve. There is a likely underlying degenerative change (Barlow disease) with thickened leaflets. There is a large mass at the base of the posterior leaflet (right of the image). A large mass can also be seen attached to the anterior leaflet (right of the image). In the still frame—obtained in diastole—the vegetations are shown in the left ventricle. In the associated movie clip, the vegetations can be seen attached to the leaflets. Also in the movie clip, a ruptured chord can be seen flicking into the left atrium during systole. Perforation, involving one or both leaflets, cannot be excluded. Colour flow Doppler imaging (not shown) demonstrated an eccentric jet of severe mitral regurgitation directed over the posterior leaflet. LA, left atrium; LV, left ventricle; MV, mitral valve. (If reading the pdf online, click on the image to view the video.)

Transoesophageal echocardiographic view of the left ventricular outflow tract in the mid-oesophageal long-axis view in a patient with bioprosthetic aortic valve endocarditis. Complex vegetations can be seen involving more than one bioprosthetic leaflet. There is no evidence of an aortic root abscess. AV, aortic valve; LA, left atrium; LV, left ventricle. (If reading the pdf online, click on the image to view the video.)

Transoesophageal echocardiographic mid-oesophageal four-chamber view showing mitral valve endocarditis. A large vegetation can be seen attached to the anterior mitral leaflet. There also appears to be a perforation involving anterior leaflet. The patient had very severe mitral regurgitation, and emergency surgery was required. LA, left atrium; LV, left ventricle; MV, mitral valve; RV, right ventricle. (If reading the pdf online, click on the image to view the video.)

Algorithm for diagnosing endocarditis using the modified Duke criteria, echocardiography and newer imaging techniques, including fluorodeoxyglucose positron emission tomography and radiolabelled leucocyte single-photon emission CT. The newer imaging techniques are useful when the diagnosis of endocarditis is possible but not confirmed with the modified Duke criteria or by echocardiography.
References
-
- Habib G., Lancellotti P., Antunes M.J., et al. 2015 ESC guidelines for the management of infective endocarditis: the task force for the management of infective endocarditis of the European society of cardiology (ESC) Eur Heart J. 2015;36:3075–3128. - PubMed
-
- Fernández-Hidalgo N, Almirante B, Tornos P, et al. Contemporary epidemiology and prognosis of health care-associated infective endocarditis. Clin Infect Dis. 2008;47:1287–1297. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
