

A comprehensive review of transvenous obliteration techniques in the management of gastric varices
- PMID: 36960571
- PMCID: PMC10679599
- DOI: 10.5152/dir.2022.21193
A comprehensive review of transvenous obliteration techniques in the management of gastric varices
Abstract
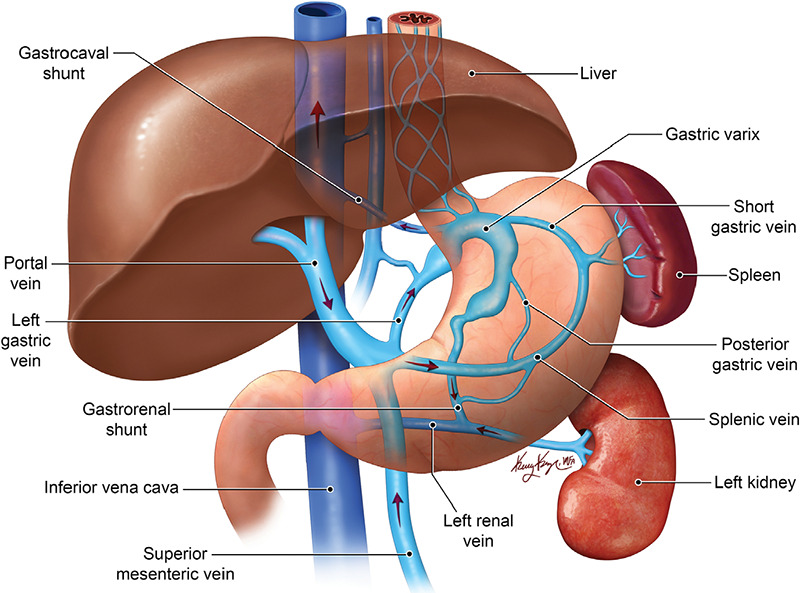
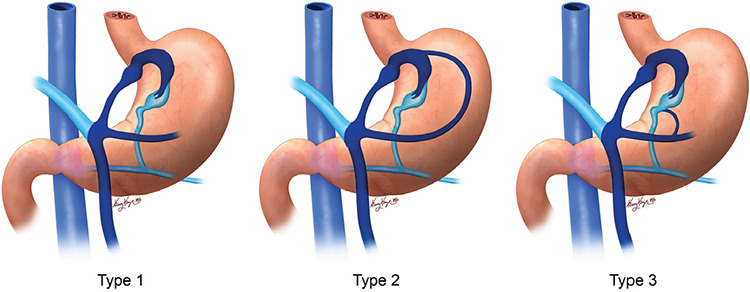
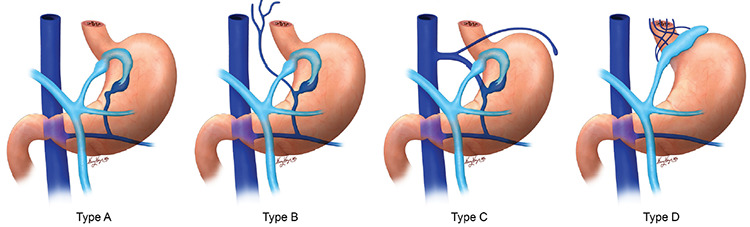
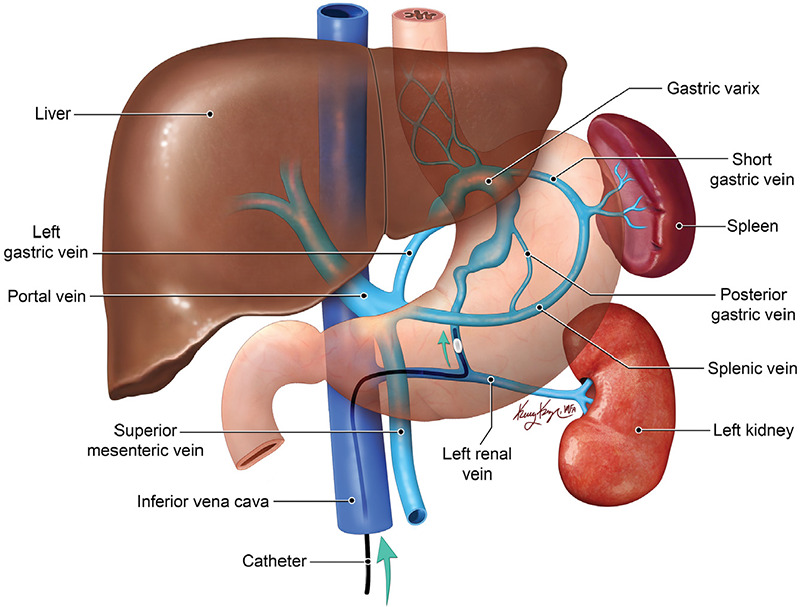
Bleeding gastric varices (GVs) is a life-threatening complication of portal hypertension, with higher morbidity and mortality rates compared with bleeding esophageal varices (EVs). The endovascular techniques for the management of GVs are mainly transjugular intrahepatic portosystemic shunt (TIPS) and transvenous obliteration of the GVs. Transvenous obliteration techniques can be an alternative or an adjunct to TIPS for treatment of GVs, depending on the clinical scenario, and are less invasive than TIPS. However, these procedures are associated with increased portal pressure and related complications, mainly worsening of the EVs. In this article, the different techniques of transvenous obliteration of GVs, their indications, contraindications, and outcomes are discussed.
Keywords: Cirrhosis; TIPS; gastric varices; transvenous obliteration; upper GI bleeding.
Conflict of interest statement
The authors declared no conflicts of interest.
Figures
References
-
- de Franchis R, Primignani M. Natural history of portal hypertension in patients with cirrhosis. Clin Liver Dis. 2001;5(3):645–663. - PubMed
-
- Sarin SK, Lahoti D, Saxena SP, Murthy NS, Makwana UK. Prevalence, classification and natural history of gastric varices: a long-term follow-up study in 568 portal hypertension patients. Hepatology. 1992;16(6):1343–1349. - PubMed
-
- Garcia-Tsao G, Abraldes JG, Berzigotti A, Bosch J. Portal hypertensive bleeding in cirrhosis: risk stratification, diagnosis, and management: 2016 practice guidance by the American Association for the study of liver diseases. Hepatology. 2017;65(1):310–335. - PubMed
-
- Ferral H, Gamboa P, Postoak DW, et al. Survival after elective transjugular intrahepatic portosystemic shunt creation: prediction with model for end-stage liver disease score. Radiology. 2004;231(1):231–236. - PubMed
-
- Montgomery A, Ferral H, Vasan R, Postoak DW. MELD score as a predictor of early death in patients undergoing elective transjugular intrahepatic portosystemic shunt (TIPS) procedures. Cardiovasc Intervent Radiol. 2005;28(3):307–312. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
