

Patterns of non-communicable comorbidities at start of tuberculosis treatment in three regions of the Philippines: The St-ATT cohort
- PMID: 36962076
- PMCID: PMC10021424
- DOI: 10.1371/journal.pgph.0000011
Patterns of non-communicable comorbidities at start of tuberculosis treatment in three regions of the Philippines: The St-ATT cohort
Abstract
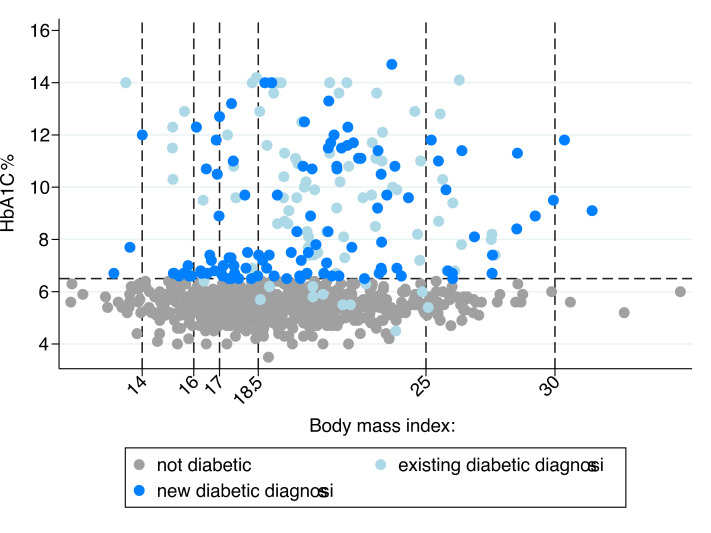
Diabetes and undernutrition are common risk factors for tuberculosis (TB), associated with poor treatment outcomes and exacerbated by TB. Limited data exist describing patterns and risk factors of multiple comorbidities in persons with TB. Nine-hundred participants (69.6% male) were enrolled in the Starting Anti-TB Treatment (St-ATT) cohort, including 133 (14.8%) initiating treatment for multi-drug resistant TB (MDR-TB). Comorbidities were defined as: diabetes, HbA1c ≥6.5% and/or on medication; hypertension, systolic blood pressure ≥140 mmHg or diastolic blood pressure ≥90 mmHg and/or on medication; anaemia (moderate/severe), haemoglobin <11g/dL; and, undernutrition (moderate/severe) body-mass-index <17 kg/m2. The most common comorbidities were undernutrition 23.4% (210/899), diabetes 22.5% (199/881), hypertension 19.0% (164/864) and anaemia 13.5% (121/899). Fifty-eight percent had ≥1 comorbid condition (496/847), with 17.1% having ≥2; most frequently diabetes and hypertension (N = 57, 6.7%). Just over half of diabetes (54.8%) and hypertension (54.9%) was previously undiagnosed. Poor glycemic control in those on medication (HbA1c≥8.0%) was common (N = 50/73, 68.5%). MDR-TB treatment was associated with increased odds of diabetes (Adjusted odds ratio (AOR) = 2.48, 95% CI: 1.55-3.95); but decreased odds of hypertension (AOR = 0.55, 95% CI: 0.39-0.78). HIV infection was only associated with anaemia (AOR = 4.51, 95% CI: 1.01-20.1). Previous TB treatment was associated with moderate/severe undernutrition (AOR = 1.98, 95% CI: 1.40-2.80), as was duration of TB-symptoms before starting treatment and household food insecurity. No associations for sex, alcohol or tobacco use were observed. MDR-TB treatment was marginally associated with having ≥2 comorbidities (OR = 1.52, 95% CI: 0.97-2.39). TB treatment programmes should plan for large proportions of persons requiring diagnosis and management of comorbidities with the potential to adversely affect TB treatment outcomes and quality of life. Dietary advice and nutritional management are components of comprehensive care for the above conditions as well as TB and should be included in planning of patient-centred services.
Copyright: © 2021 Cox et al. This is an open access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Conflict of interest statement
All authors declare no competing interests
Figures





References
-
- WHO. Global TB Report. 2020.
-
- Food and Nutrition Research Institute DoSaT, the Philippines,. 8th National Nutrition Survey2015 12th Jan 2019. Available from: http://www.fnri.dost.gov.ph/index.php/nutrition-statistic/19-nutrition-s....
-
- Mendenhall E, Kohrt BA, Norris SA, Ndetei D, Prabhakaran D. Non-communicable disease syndemics: poverty, depression, and diabetes among low-income populations. Lancet. 2017;389(10072):951–63. Epub 2017/03/09. doi: 10.1016/S0140-6736(17)30402-6 ; PubMed Central PMCID: PMC5491333. - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources