

The global burden of tuberculous meningitis in adults: A modelling study
- PMID: 36962116
- PMCID: PMC10021871
- DOI: 10.1371/journal.pgph.0000069
The global burden of tuberculous meningitis in adults: A modelling study
Abstract
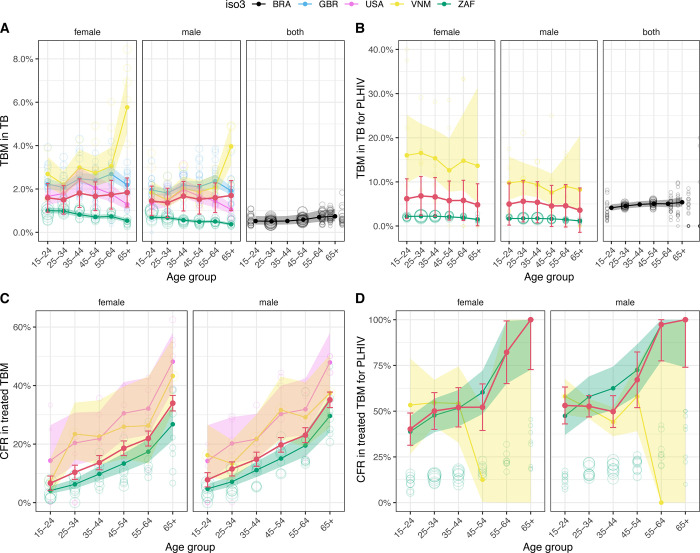
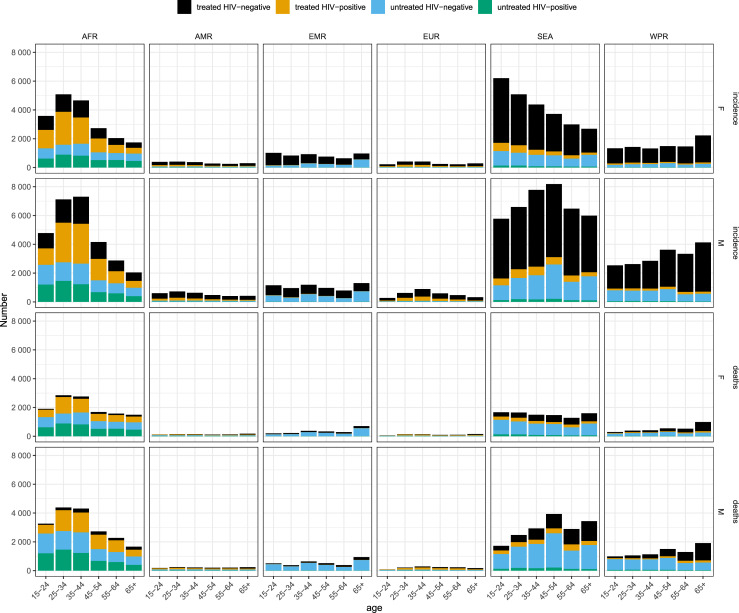
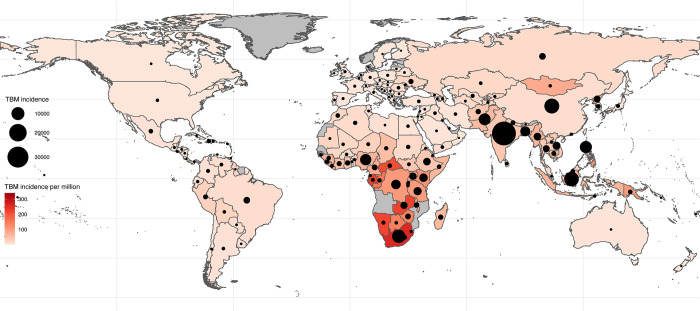
Tuberculous meningitis (TBM) is the most lethal form of tuberculosis. The incidence and mortality of TBM is unknown due to diagnostic challenges and limited disaggregated reporting of treated TBM by existing surveillance systems. We aimed to estimate the incidence and mortality of TBM in adults (15+ years) globally. Using national surveillance data from Brazil, South Africa, the United Kingdom, the United States of America, and Vietnam, we estimated the fraction of reported tuberculosis that is TBM, and the case fatality ratios for treated TBM in each of these countries. We adjusted these estimates according to findings from a systematic review and meta-analysis and applied them to World Health Organization tuberculosis notifications and estimates to model the global TBM incidence and mortality. Assuming the case detection ratio (CDR) for TBM was the same as all TB, we estimated that in 2019, 164,000 (95% UI; 129,000-199,000) adults developed TBM globally; 23% were among people living with HIV. Almost 60% of incident TBM occurred in males and 20% were in adults 25-34 years old. 70% of global TBM incidence occurred in Southeast Asia and Africa. We estimated that 78,200 (95% UI; 52,300-104,000) adults died of TBM in 2019, representing 48% of incident TBM. TBM case fatality in those treated was on average 27%. Sensitivity analysis assuming improved detection of TBM compared to other forms of TB (CDR odds ratio of 2) reduced estimated global mortality to 54,900 (95% UI; 32,200-77,700); assuming instead worse detection for TBM (CDR odds ratio of 0.5) increased estimated mortality to 125,000 (95% UI; 88,800-161,000). Our results highlight the need for improved routine TBM monitoring, especially in high burden countries. Reducing TBM incidence and mortality will be necessary to achieve the End TB Strategy targets.
Copyright: © 2021 Dodd et al. This is an open access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures

References
Grants and funding
LinkOut - more resources
Full Text Sources