

Retention on ART and viral suppression among patients in alternative models of differentiated HIV service delivery in KwaZulu-Natal, South Africa
- PMID: 36962695
- PMCID: PMC10021436
- DOI: 10.1371/journal.pgph.0000336
Retention on ART and viral suppression among patients in alternative models of differentiated HIV service delivery in KwaZulu-Natal, South Africa
Erratum in
-
Correction: Retention on ART and viral suppression among patients in alternative models of differentiated HIV service delivery in KwaZulu-Natal, South Africa.PLOS Glob Public Health. 2024 Mar 8;4(3):e0003038. doi: 10.1371/journal.pgph.0003038. eCollection 2024. PLOS Glob Public Health. 2024. PMID: 38457417 Free PMC article.
Abstract
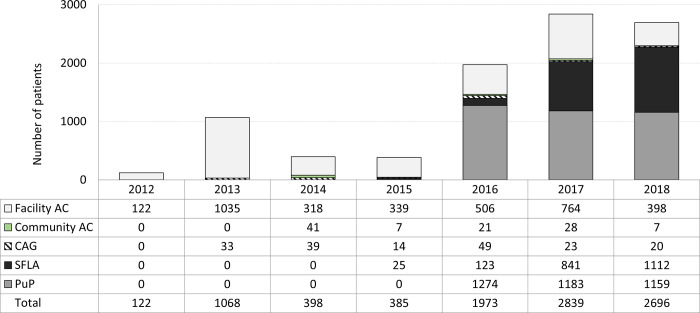
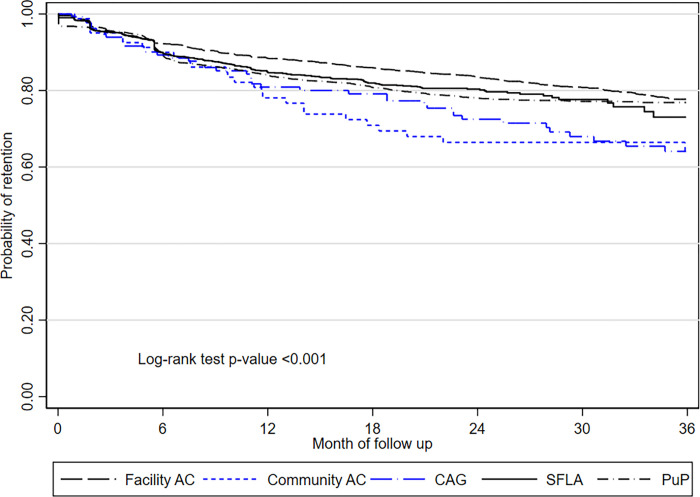
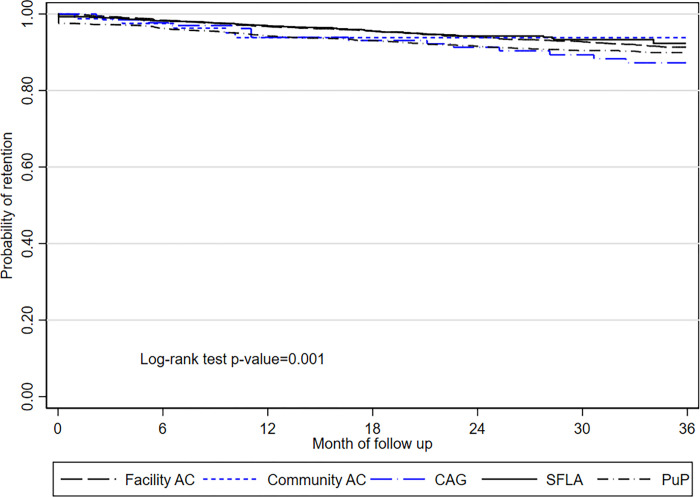
Differentiated models of HIV care (DMOC) aim to improve health care efficiency. We describe outcomes of five DMOC in KwaZulu-Natal, South Africa: facility adherence clubs (facility AC) and community adherence clubs (community AC), community antiretroviral treatment (ART) groups (CAG), spaced fast lane appointments (SFLA), and community pick up points (PuP). This retrospective cohort study included 8241 eligible patients enrolled into DMOC between 1/1/2012 and 31/12/2018. We assessed retention in DMOC and on ART, and viral load suppression (<1000 copies/mL). Kaplan-Meier techniques were applied to describe crude retention. Mixed effects parametric survival models with Weibull distribution and clustering on health center and individual levels were used to assess predictors for ART and DMOC attrition, and VL rebound (≥1000 copies/mL). Overall DMOC retention was 85%, 80%, and 76% at 12, 24 and 36 months. ART retention at 12, 24 and 36 months was 96%, 93%, 90%. Overall incidence rate of VL rebound was 1.9 episodes per 100 person-years. VL rebound rate was 4.9 episodes per 100 person-years among those enrolled in 2012-2015, and 0.8 episodes per 100 person-years among those enrolled in 2016-2018 (RR 0.12; 95% CI, 0.09-0.15, p<0.001). Prevalence of confirmed virological failure was 0.6% (38/6113). Predictors of attrition from DMOC and from ART were male gender, younger age, shorter duration on ART before enrollment. Low level viremia (>200-399 copies/mL) was associated with higher hazards of VL rebound and attrition from ART. Concurrent implementation of several DMOC in a large ART program is feasible and can achieve sustained retention on ART and VL suppression.
Copyright: © 2022 Shigayeva et al. This is an open access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
Similar articles
-
Outcomes of patients on second- and third-line ART enrolled in ART adherence clubs in Maputo, Mozambique.Trop Med Int Health. 2020 Dec;25(12):1496-1502. doi: 10.1111/tmi.13490. Epub 2020 Oct 14. Trop Med Int Health. 2020. PMID: 32959934 Free PMC article.
-
Adherence clubs and decentralized medication delivery to support patient retention and sustained viral suppression in care: Results from a cluster-randomized evaluation of differentiated ART delivery models in South Africa.PLoS Med. 2019 Jul 23;16(7):e1002874. doi: 10.1371/journal.pmed.1002874. eCollection 2019 Jul. PLoS Med. 2019. PMID: 31335865 Free PMC article. Clinical Trial.
-
High rates of retention and viral suppression in the scale-up of antiretroviral therapy adherence clubs in Cape Town, South Africa.J Int AIDS Soc. 2017 Jul 21;20(Suppl 4):21649. doi: 10.7448/IAS.20.5.21649. J Int AIDS Soc. 2017. PMID: 28770595 Free PMC article.
-
HIV viral suppression and longevity among a cohort of children initiating antiretroviral therapy in Eastern Cape, South Africa.J Int AIDS Soc. 2018 Aug;21(8):e25168. doi: 10.1002/jia2.25168. J Int AIDS Soc. 2018. PMID: 30094952 Free PMC article.
-
Differentiated models of care for postpartum women on antiretroviral therapy in Cape Town, South Africa: a cohort study.J Int AIDS Soc. 2017 Jul 21;20(Suppl 4):21636. doi: 10.7448/IAS.20.5.21636. J Int AIDS Soc. 2017. PMID: 28770593 Free PMC article.
Cited by
-
HIV care retention in three multi-month ART dispensing: a retrospective cohort study in Mozambique.AIDS. 2024 Jul 15;38(9):1402-1411. doi: 10.1097/QAD.0000000000003913. Epub 2024 May 3. AIDS. 2024. PMID: 38652496 Free PMC article.
-
Prevalence and trends of advanced HIV disease among antiretroviral therapy-naïve and antiretroviral therapy-experienced patients in South Africa between 2010-2021: a systematic review and meta-analysis.BMC Infect Dis. 2023 Aug 22;23(1):549. doi: 10.1186/s12879-023-08521-4. BMC Infect Dis. 2023. PMID: 37608300 Free PMC article.
-
Correction: Retention on ART and viral suppression among patients in alternative models of differentiated HIV service delivery in KwaZulu-Natal, South Africa.PLOS Glob Public Health. 2024 Mar 8;4(3):e0003038. doi: 10.1371/journal.pgph.0003038. eCollection 2024. PLOS Glob Public Health. 2024. PMID: 38457417 Free PMC article.
-
Understanding health outcome drivers among adherence club patients in clinics of Gauteng, South Africa: a structural equation modelling (SEM) approach.AIDS Res Ther. 2023 Oct 5;20(1):71. doi: 10.1186/s12981-023-00565-5. AIDS Res Ther. 2023. PMID: 37798794 Free PMC article.
-
'Not taking medications and taking medication, it was the same thing:' perspectives of antiretroviral therapy among people hospitalised with advanced HIV disease.BMC Infect Dis. 2024 Aug 13;24(1):819. doi: 10.1186/s12879-024-09729-8. BMC Infect Dis. 2024. PMID: 39138390 Free PMC article.
References
-
- Vandendyck Mr M, Motsamai M, Mubanga M, Makhakhe S, Jonckheree S, Shroufi A, et al. Community antiretroviral therapy groups (CAGs) in Nazareth, Lesotho: the way forward for an effective community model for HIV care? 20th International AIDS Conference, July 20–25, 2014, Melbourne, Australia. 2014;
LinkOut - more resources
Full Text Sources