

Reactive focal drug administration associated with decreased malaria transmission in an elimination setting: Serological evidence from the cluster-randomized CoRE study
- PMID: 36962857
- PMCID: PMC10021141
- DOI: 10.1371/journal.pgph.0001295
Reactive focal drug administration associated with decreased malaria transmission in an elimination setting: Serological evidence from the cluster-randomized CoRE study
Abstract
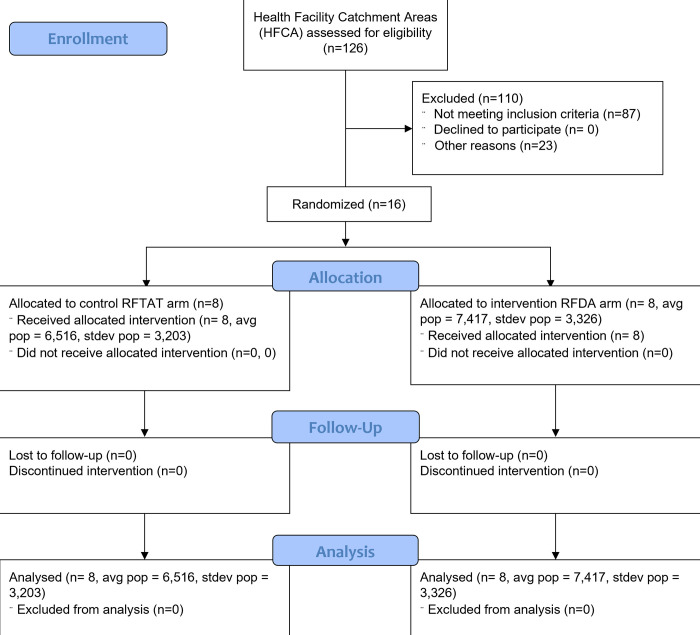
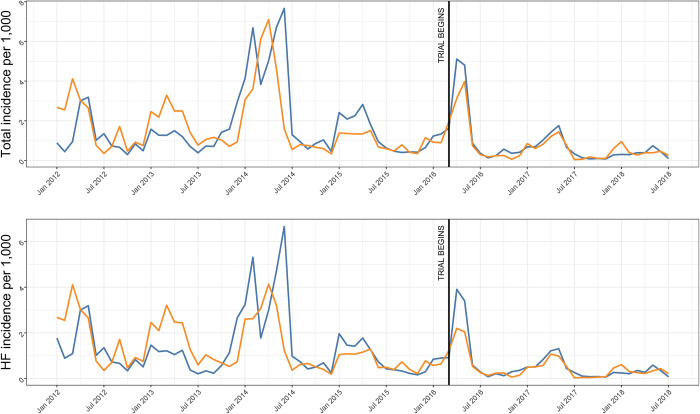
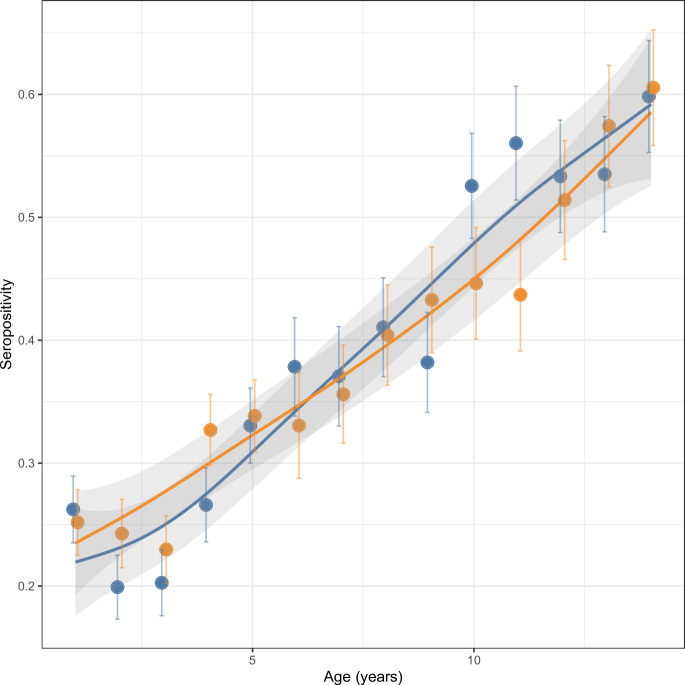
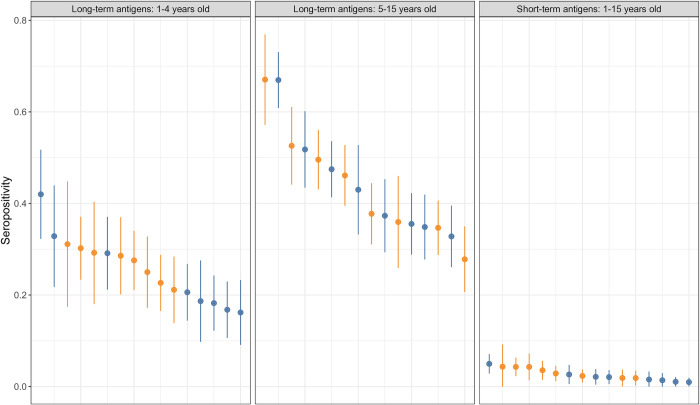
Efforts to eliminate malaria transmission need evidence-based strategies. However, accurately assessing end-game malaria elimination strategies is challenging due to the low level of transmission and the rarity of infections. We hypothesised that presumptively treating individuals during reactive case detection (RCD) would reduce transmission and that serology would more sensitively detect this change over standard approaches. We conducted a cluster randomised control trial (NCT02654912) of presumptive reactive focal drug administration (RFDA-intervention) compared to the standard of care, reactive focal test and treat (RFTAT-control) in Southern Province, Zambia-an area of low seasonal transmission (overall incidence of ~3 per 1,000). We measured routine malaria incidence from health facilities as well as PCR parasite prevalence / antimalarial seroprevalence in an endline cross-sectional population survey. No significant difference was identified from routine incidence data and endline prevalence by polymerase chain reaction (PCR) had insufficient numbers of malaria infections (i.e., 16 infections among 6,276 children) to assess the intervention. Comparing long-term serological markers, we found a 19% (95% CI = 4-32%) reduction in seropositivity for the RFDA intervention using a difference in differences approach incorporating serological positivity and age. We also found a 37% (95% CI = 2-59%) reduction in seropositivity to short-term serological markers in a post-only comparison. These serological analyses provide compelling evidence that RFDA both has an impact on malaria transmission and is an appropriate end-game malaria elimination strategy. Furthermore, serology provides a more sensitive approach to measure changes in transmission that other approaches miss, particularly in very low transmission settings. Trial Registration: Registered at www.clinicaltrials.gov (NCT02654912, 13/1/2016).
Copyright: © 2022 Bridges et al. This is an open access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
Associated data
LinkOut - more resources
Full Text Sources
Medical