

The availability of essential medicines for cardiovascular diseases at healthcare facilities in low- and middle-income countries: The case of Bangladesh
- PMID: 36962886
- PMCID: PMC10021517
- DOI: 10.1371/journal.pgph.0001154
The availability of essential medicines for cardiovascular diseases at healthcare facilities in low- and middle-income countries: The case of Bangladesh
Abstract
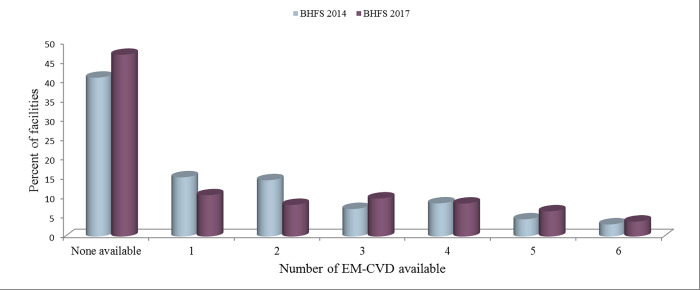
Long-term, often lifelong care for cardiovascular disease (CVD) patients requires consistent use of medicine; hence, the availability of essential medicine for CVD (EM-CVD) is vital for treatment, quality of life, and survival. We aimed to assess the availability of EM-CVD and explore healthcare facility (HCF) characteristics associated with the availability of those medicines in Bangladesh. This study utilized publicly available cross-sectional data from the 2014 and 2017 waves of the Bangladesh Health Facilities Survey (BHFS). The analysis included 204 facilities (84 from the 2014 BHFS and 120 from the 2017 BHFS) that provide CVD diagnosis and treatment services. The outcome variable "EM-CVD availability" was calculated as a counting score of the following tracer medicines: angiotensin-converting enzyme (ACE) inhibitors (enalapril), thiazide, beta-blockers (atenolol), calcium channel blockers (amlodipine and nifedipine), aspirin, and simvastatin/atorvastatin. A multivariable Poisson regression model was used to identify the HCF characteristics associated with EM-CVD availability. The number of Bangladeshi HCFs that provide CVD screening and treatment services increased just a little between 2014 and 2017 (from 5.4% to 7.9%). Since 2014, there has been an increase in the availability of calcium channel blockers (from 37.5% to 38.5%), aspirin (from 25.3% to 27.9%), and simvastatin/atorvastatin (from 8.0% to 30.7%), whereas there has been a decrease in the availability of ACE inhibitors (enalapril) (from 12.5% to 6.5%), thiazide (from 15.7% to 11.1%), and beta-blockers (from 42.5% to 32.5%). The likelihood of EM-CVD being available was higher among private and urban facilities than among public and rural facilities. Furthermore, facilities that had 24-hour staff coverage and performed quality assurance activities had a higher chance of having EM-CVD available than those that did not have 24-hour staff coverage and did not undertake quality assurance activities. Government authorities should think about a wide range of policy implications, such as putting more emphasis on public and rural facilities, making sure staff is available 24 hours a day, and performing quality assurance activities at facilities to make EM-CVD more available.
Copyright: © 2022 Hakim et al. This is an open access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures


References
-
- Organization WH. (2021) Cardiovascular diseases (CVDs) Key facts.
-
- Bloom DE, Cafiero E, Jané-Llopis E, Abrahams-Gessel S, Bloom LR, et al. (2012) The global economic burden of noncommunicable diseases. Program on the Global Demography of Aging.
-
- Bloom DE, Chisholm D, Jané-Llopis E, Prettner K, Stein A, et al. (2011) From burden to" best buys": reducing the economic impact of non-communicable disease in low-and middle-income countries. Program on the Global Demography of Aging.
LinkOut - more resources
Full Text Sources
Miscellaneous