

A Type II hybrid effectiveness-implementation study of an integrated CHW intervention to address maternal healthcare in rural Nepal
- PMID: 36963046
- PMCID: PMC10021605
- DOI: 10.1371/journal.pgph.0001512
A Type II hybrid effectiveness-implementation study of an integrated CHW intervention to address maternal healthcare in rural Nepal
Abstract
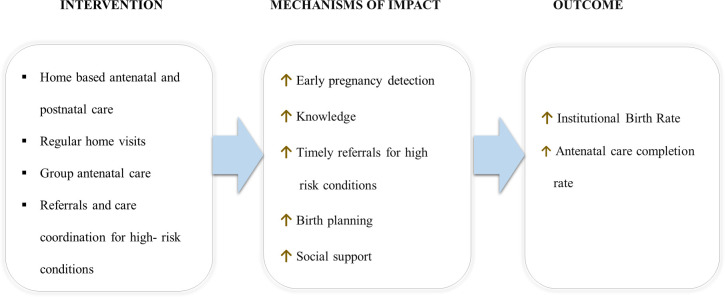
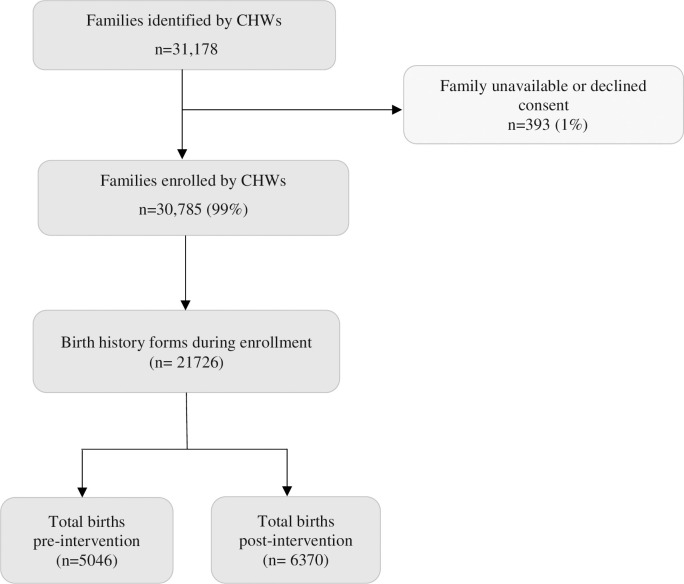
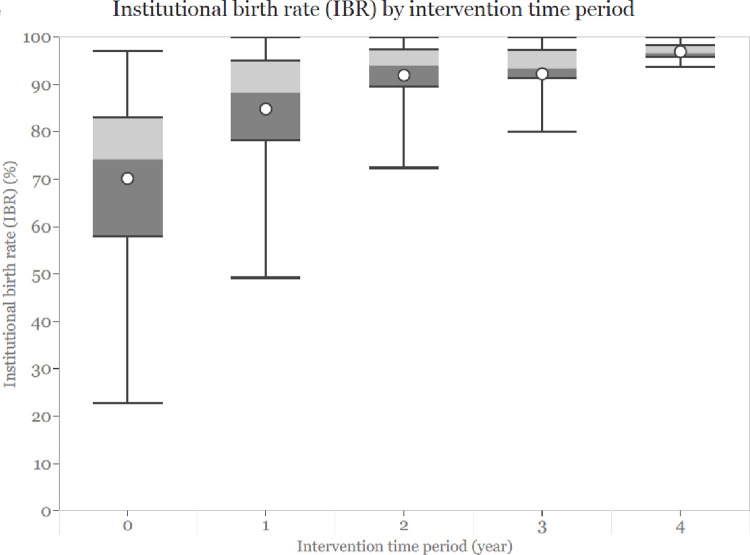
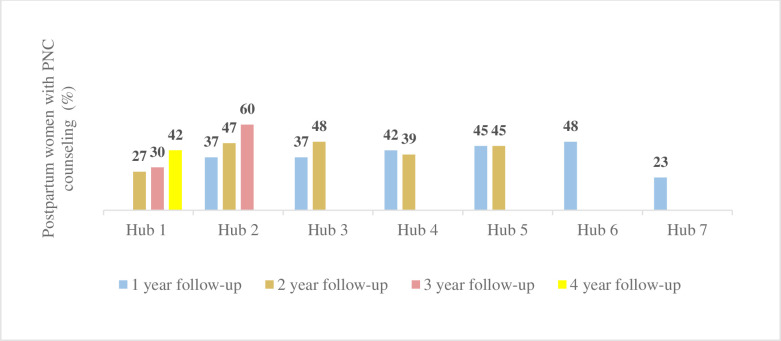
Skilled care during pregnancy, childbirth, and postpartum is essential to prevent adverse maternal health outcomes, yet utilization of care remains low in many resource-limited countries, including Nepal. Community health workers (CHWs) can mitigate health system challenges and geographical barriers to achieving universal health coverage. Gaps remain, however, in understanding whether evidence-based interventions delivered by CHWs, closely aligned with WHO recommendations, are effective in Nepal's context. We conducted a type II hybrid effectiveness-implementation, mixed-methods study in two rural districts in Nepal to evaluate the effectiveness and the implementation of an evidence-based integrated maternal and child health intervention delivered by CHWs, using a mobile application. The intervention was implemented stepwise over four years (2014-2018), with 65 CHWs enrolling 30,785 families. We performed a mixed-effects Poisson regression to assess institutional birth rate (IBR) pre-and post-intervention. We used the Reach, Effectiveness, Adoption, Implementation, and Maintenance framework to evaluate the implementation during and after the study completion. There was an average 30% increase in IBR post-intervention, adjusting for confounding variables (p<0.0001). Study enrollment showed 35% of families identified as dalit, janjati, or other castes. About 78-89% of postpartum women received at least one CHW-counseled home visit within 60 days of childbirth. Ten (53% of planned) municipalities adopted the intervention during the study period. Implementation fidelity, measured by median counseled home visits, improved with intervention time. The intervention was institutionalized beyond the study period and expanded to four additional hubs, albeit with adjustments in management and supervision. Mechanisms of intervention impact include increased knowledge, timely referrals, and longitudinal CHW interaction. Full-time, supervised, and trained CHWs delivering evidence-based integrated care appears to be effective in improving maternal healthcare in rural Nepal. This study contributes to the growing body of evidence on the role of community health workers in achieving universal health coverage.
Copyright: © 2023 Tiwari et al. This is an open access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Conflict of interest statement
I have read the journal’s policy and the authors of this manuscript have the following competing interests: A. Tiwari and A. Thapa are employed by a US-based non-profit (Possible) and based in Nepal. S. Sapkota and R. Khatri are employed by a Nepal-based non-governmental organization, Possible that operates with support from US-based Possible. VB, BB, HJR, R. Paudel, SG, NM, R. Poudel and LDB are employed by a Nepal-based non-governmental organization (Nyaya Health Nepal) that delivers free healthcare in rural Nepal using funds from the Government of Nepal and other public, philanthropic, and private foundation sources. NC, DM, SM are employed by, and SM, DC, DM, and S. Sapkota are faculty members at a private medical school (Icahn School of Medicine at Mount Sinai). DM is a member on US-based Possible’s Board of Directors, for which he receives no compensation. IB is a board chair of Nepal-based Possible. WW is a faculty member at a private university (Boston University School of Medicine). DC is a faculty member and SH is a graduate student at a public university (University of Washington). R. Schwarz is employed at an academic medical center (Brigham and Women’s Hospital) that receives public sector research funding, as well as revenue through private sector fee-for-service medical transactions and private foundation grants. R. Schwarz is a faculty member at a private medical school (Harvard Medical School) and employed at an academic medical center (Massachusetts General Hospital) that receives public sector research funding, as well as revenue through private sector fee-for-service medical transactions and private foundation grants. SA is a faculty member at a private medical school (NYU School of Medicine). SK is a nursing student at Gandaki Medical College Teaching Hospital and Research Center. IN is a graduate student at a private university (Harvard T.H. Chan School of Public Health). LK is employed by a non-profit (Medic). PT is a graduate student at a public university (University of New South Wales). S. Saud is employed by a government hospital of Nepal (Civil Service Hospital). YKBK is employed by a government hospital of Nepal (COVID Hospital in Shikhar municipality). AB is employed by the local government of Nepal (Amargadhi municipality). R. Shrestha and KRM are employed by a non-profit hospital (Dhulikhel Hospital, Kathmandu University Hospital). R. Kafle is employed by a Nepal-based non-profit (Nick Simons Institute). GNS is a director of the Nursing and Social Security Division under the Government of Nepal Ministry of Health and Population. All authors declare that we have no competing financial interests.
Figures

Similar articles
-
An integrated community health worker intervention in rural Nepal: a type 2 hybrid effectiveness-implementation study protocol.Implement Sci. 2018 Mar 29;13(1):53. doi: 10.1186/s13012-018-0741-x. Implement Sci. 2018. PMID: 29598824 Free PMC article.
-
An integrated intervention for chronic care management in rural Nepal: protocol of a type 2 hybrid effectiveness-implementation study.Trials. 2020 Jan 29;21(1):119. doi: 10.1186/s13063-020-4063-3. Trials. 2020. PMID: 31996250 Free PMC article.
-
Working with community health workers to improve maternal and newborn health outcomes: implementation and scale-up lessons from eastern Uganda.Glob Health Action. 2017 Aug;10(sup4):1345495. doi: 10.1080/16549716.2017.1345495. Glob Health Action. 2017. PMID: 28849718 Free PMC article.
-
Effects of community health worker interventions on socioeconomic inequities in maternal and newborn health in low-income and middle-income countries: a mixed-methods systematic review.BMJ Glob Health. 2019 Jun 16;4(3):e001308. doi: 10.1136/bmjgh-2018-001308. eCollection 2019. BMJ Glob Health. 2019. PMID: 31275619 Free PMC article.
-
Multilevel determinants of community health workers for an effective maternal and child health programme in sub-Saharan Africa: a systematic review.BMJ Glob Health. 2022 Apr;7(4):e008162. doi: 10.1136/bmjgh-2021-008162. BMJ Glob Health. 2022. PMID: 35393287 Free PMC article.
Cited by
-
Community health workers' barriers and facilitators to use a novel mHealth tool for motivational interviewing to improve adherence to care among youth living with HIV in rural Nepal.PLOS Glob Public Health. 2024 Jul 11;4(7):e0002911. doi: 10.1371/journal.pgph.0002911. eCollection 2024. PLOS Glob Public Health. 2024. PMID: 38990929 Free PMC article.
References
-
- World Health Organization. Trends in maternal mortality 2000 to 2017: estimates by WHO, UNICEF, UNFPA, World Bank Group and the United Nations Population Division: executive summary. Geneva: World Health Organization; 2019 2019. Contract No.: WHO/RHR/19.23.
-
- Teferra AS, Alemu FM, Woldeyohannes SM. Institutional delivery service utilization and associated factors among mothers who gave birth in the last 12 months in Sekela District, North West of Ethiopia: A community—based cross sectional study. BMC Pregnancy and Childbirth. 2012;12(1):74. doi: 10.1186/1471-2393-12-74 - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources