

National health policies and strategies for addressing chronic kidney disease: Data from the International Society of Nephrology Global Kidney Health Atlas
- PMID: 36963092
- PMCID: PMC10021302
- DOI: 10.1371/journal.pgph.0001467
National health policies and strategies for addressing chronic kidney disease: Data from the International Society of Nephrology Global Kidney Health Atlas
Abstract
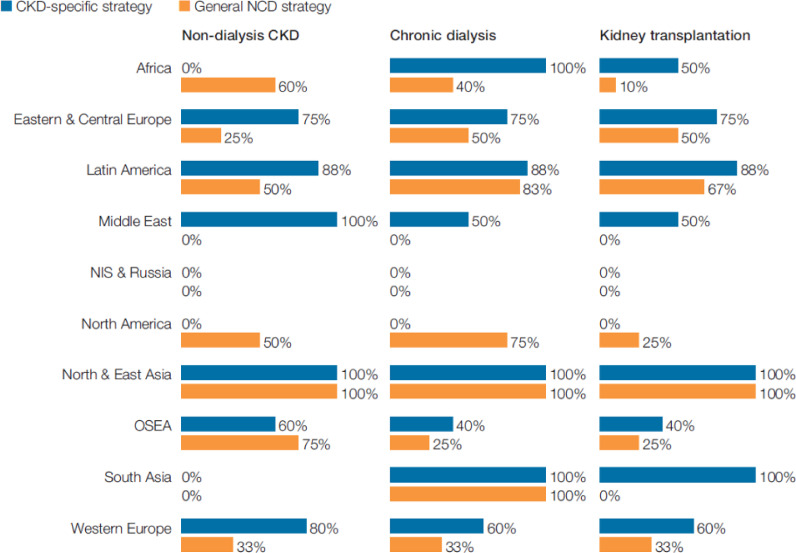
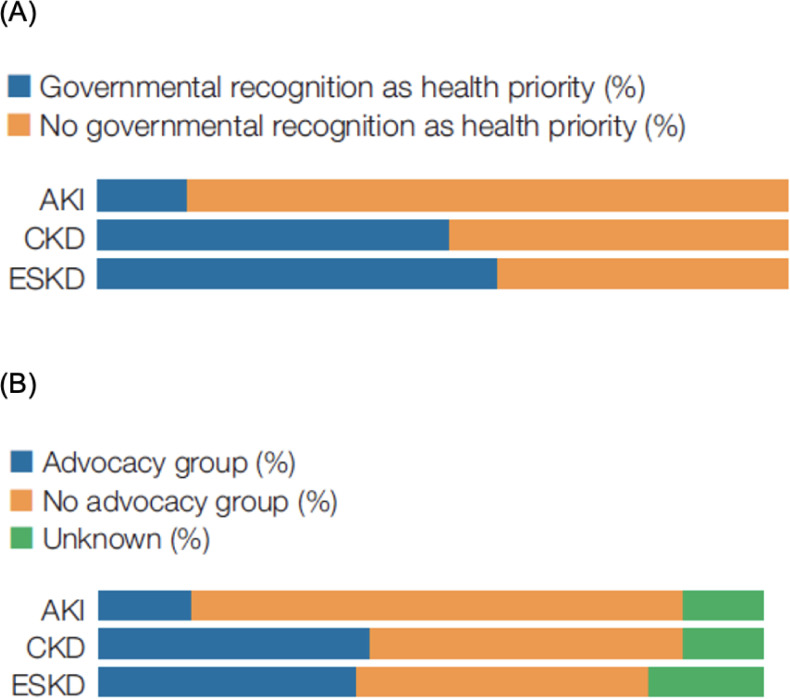
National strategies for addressing chronic kidney disease (CKD) are crucial to improving kidney health. We sought to describe country-level variations in non-communicable disease (NCD) strategies and CKD-specific policies across different regions and income levels worldwide. The International Society of Nephrology Global Kidney Health Atlas (GKHA) was a multinational cross-sectional survey conducted between July and October 2018. Responses from key opinion leaders in each country regarding national NCD strategies, the presence and scope of CKD-specific policies, and government recognition of CKD as a health priority were described overall and according to region and income level. 160 countries participated in the GKHA survey, comprising 97.8% of the world's population. Seventy-four (47%) countries had an established national NCD strategy, and 53 (34%) countries reported the existence of CKD-specific policies, with substantial variation across regions and income levels. Where CKD-specific policies existed, non-dialysis CKD care was variably addressed. 79 (51%) countries identified government recognition of CKD as a health priority. Low- and low-middle income countries were less likely to have strategies and policies for addressing CKD and have governments which recognise it as a health priority. The existence of CKD-specific policies, and a national NCD strategy more broadly, varied substantially across different regions around the world but was overall suboptimal, with major discrepancies between the burden of CKD in many countries and governmental recognition of CKD as a health priority. Greater recognition of CKD within national health policy is critical to improving kidney healthcare globally.
Copyright: © 2023 Neuen et al. This is an open access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Conflict of interest statement
Outside the submitted work, BLN has received fees for advisory boards, scientific presentations, steering committee roles and travel support from AstraZeneca, Bayer, Boehringer and Ingelheim, and Janssen with all honoraria paid to his institution; AL and serves as a scientific advisor to Boehringer Ingelheim, AstraZeneca, and the National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK); is on the data safety and monitoring board for the NIDDK, Kidney Precision Medicine, University of Washington Kidney Research Institute Scientific Advisory Committee; is funded by the Canadian Institute of Health Research and Kidney Foundation of Canada; PH reports grants from Chiesi Pharmaceuticals; VJ has research grants from Baxter, GSK and reports Consultancy and Advisory Board honoraria from Baxter Healthcare, and AstraZeneca; KK-Z has received honoraria and/or support from Abbott, Abbvie, ACI Clinical (Cara Therapeutics), Akebia, Alexion, Amgen, Ardelyx, ASN (American Society of Nephrology), Astra-Zeneca, Aveo, BBraun, Chugai, Cytokinetics, Daiichi, DaVita, Fresenius, Genentech, GSK, Haymarket Media, Hofstra Medical School, IFKF (International Federation of Kidney Foundations), ISH (International Society of Hemodialysis), International Society of Renal Nutrition & Metabolism (ISRNM), JSDT (Japanese Society of Dialysis Therapy), Hospira, Kabi, Keryx, Kissei, Novartis, Novo-Nordisk, OPKO, NIH (National Institutes of Health), NKF (National Kidney Foundations), Pfizer, Regulus, Relypsa, Resverlogix, Dr Schaer, Sandoz, Sanofi, Shire, VA (Veterans’ Affairs), Takeda, Vifor, UpToDate, ZS-Pharma; PGK reports conference attendance support from Amgen Australia and honorarium from Bayer Australia; SK is Director of the Real World Evidence Consortium that conducts investigator initiated industry funded projects (Allergan, Purdue, GSK, CSL, Lundbeck, NovoNordisk, Jansen, Bayer); CPK has received consulting fees from Abbott, Akebia, Astra-Zeneca, Bayer, Cara Therapeutics, CSL Behring, Rockwell and Vifor; JP reports grants and personal fees from Baxter Healthcare, Fresenius Medical Care, and Davita Healthcare partner; RTK reports personal fees from Baxter; AY-MW reports grants from Sanofi and Otsuka; MHZ has been a consultant or advisory committee member for GSK, AstraZeneca, Roche, and Bayer; KJJ reports personal fees from Fresenius Medical Care; VP has received fees for advisory boards, steering committee roles, or scientific presentations from AbbVie, Astellas, AstraZeneca, Bayer, Baxter, BMS, Boehringer Ingelheim, Dimerix, Durect, Eli Lilly, Gilead, GSK, Janssen, Merck, Mitsubishi Tanabe, Mundipharma, Novartis, Novo Nordisk, Pfizer, Pharmalink, Relypsa, Retrophin, Sanofi, Servier, Tricida, and Vifor. MT reports grants from the Canadian Institutes for Health Research during conduct of the study; DWJ has received consultancy fees, research grants, speaker’s honoraria and travel sponsorships from Baxter Healthcare and Fresenius Medical Care, consultancy fees from Astra Zeneca, Bayer, and AWAK, speaker’s honoraria from ONO and BI & Lilly, and travel sponsorships from Ono and Amgen. He is a current recipient of an Australian National Health and Medical Research Council Leadership Investigator Grant.
Figures
References
-
- Kalantar-Zadeh K, Jafar TH, Nitsch D, Neuen BL, Perkovic V. Chronic kidney disease. The Lancet. 2021. - PubMed
-
- Foreman KJ, Marquez N, Dolgert A, Fukutaki K, Fullman N, McGaughey M, et al.. Forecasting life expectancy, years of life lost, and all-cause and cause-specific mortality for 250 causes of death: reference and alternative scenarios for 2016–40 for 195 countries and territories. The Lancet. 2018;392(10159):2052–90. doi: 10.1016/S0140-6736(18)31694-5 - DOI - PMC - PubMed
-
- Xie Y, Bowe B, Mokdad AH, Xian H, Yan Y, Li T, et al.. Analysis of the Global Burden of Disease study highlights the global, regional, and national trends of chronic kidney disease epidemiology from 1990 to 2016. Kidney international. 2018;94(3):567–81. - PubMed