

Comparison of Single-Level Posterior Cervical Foraminotomy to Anterior Cervical Discectomy and Fusion for Radiculopathy
- PMID: 36963811
- PMCID: PMC10312152
- DOI: 10.14444/8447
Comparison of Single-Level Posterior Cervical Foraminotomy to Anterior Cervical Discectomy and Fusion for Radiculopathy
Abstract
Background: Posterior cervical foraminotomy (PCF) and anterior cervical discectomy and fusion (ACDF) are 2 commonly used surgical approaches to address cervical radiculopathy. Demonstrating superiority in clinical outcomes and durability of one of the approaches could change clinical practice on a large scale. This is the largest reported single-institutional retrospective cohort of single-level PCFs compared with single-level ACDFs for cervical radiculopathy.
Methods: Patients undergoing either ACDF or PCF between 2014 and 2021 were identified using Current Procedural Terminology codes. Medical records were reviewed for demographics, surgical characteristics, and reoperations. Statistical analysis included t tests for continuous characteristics and c2 testing for categorical characteristics.
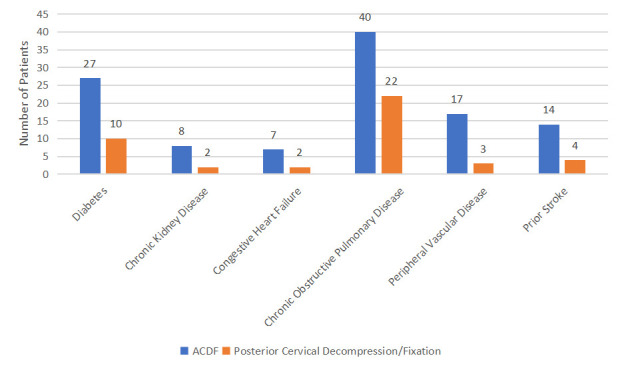
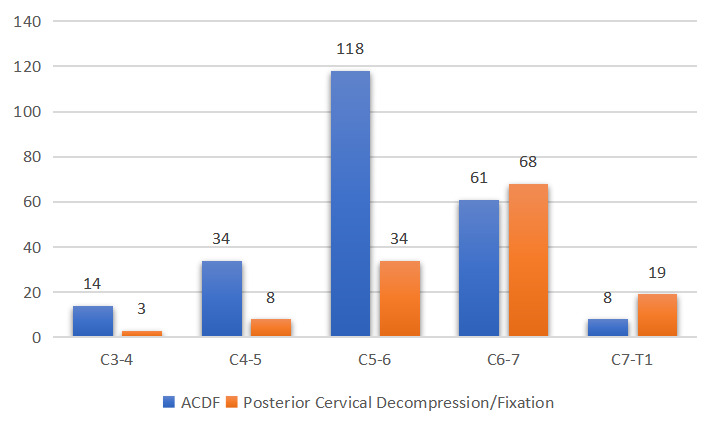
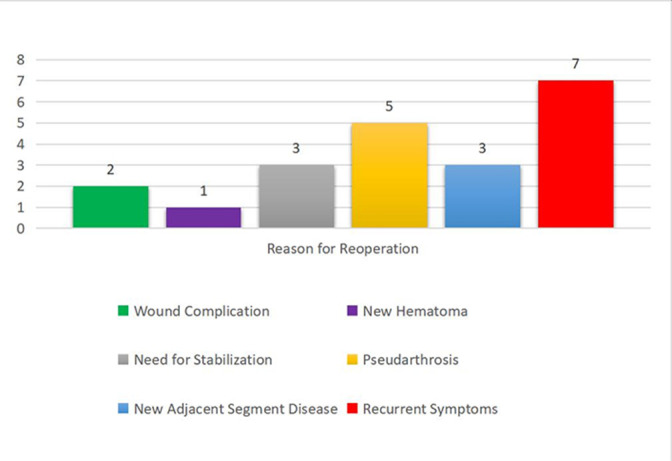
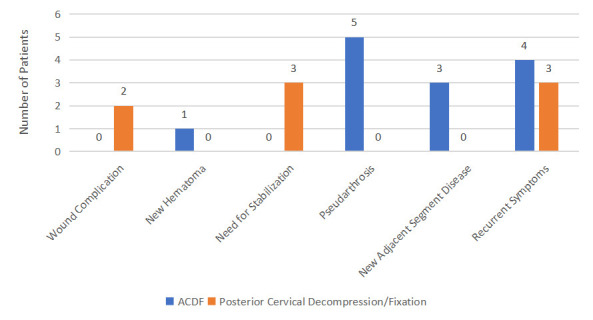
Results: In total, 236 single-level ACDFs and 138 single-level PCFs were included. There was no significant difference in age (51.0 vs 51.3 years), body mass index (BMI; 28.6 vs 28.1), or Charlson Comorbidity Index (1.89 vs 1.68) between patients who underwent ACDF and those who underwent PCF. There was no difference in the rate of reoperation (5.1% vs 5.1%), time to reoperation (247 vs 319 days), or reoperation for recurrent symptoms (1.7% vs 2.9%) for ACDF vs PCF. Hospital length of stay (LOS) was longer for ACDF compared with PCF (1.65 vs 1.35 days, P = 0.041), and the overall readmission rate after ACDF was 20.8% vs 10.9% after PCF (P = 0.014).
Conclusions: Overall reoperation rates or reoperation for recurrent symptoms between ACDF and PCF were not significantly different, demonstrating that either procedure effectively addresses the indication for surgery. There was a significantly longer LOS after ACDF than PCF, and readmission rates at 90 days and 1 year were higher after ACDF.
Keywords: anterior cervical discectomy and fusion; posterior cervical foraminotomy; radiculopathy; readmission; reoperation.
This manuscript is generously published free of charge by ISASS, the International Society for the Advancement of Spine Surgery. Copyright © 2023 ISASS. To see more or order reprints or permissions, see http://ijssurgery.com.
Conflict of interest statement
Declaration of Conflicting Interests : The authors report no conflicts of interest in this work.
Figures
References
LinkOut - more resources
Full Text Sources
Miscellaneous