

How I personalize fluid therapy in septic shock?
- PMID: 36964573
- PMCID: PMC10039545
- DOI: 10.1186/s13054-023-04363-3
How I personalize fluid therapy in septic shock?
Abstract
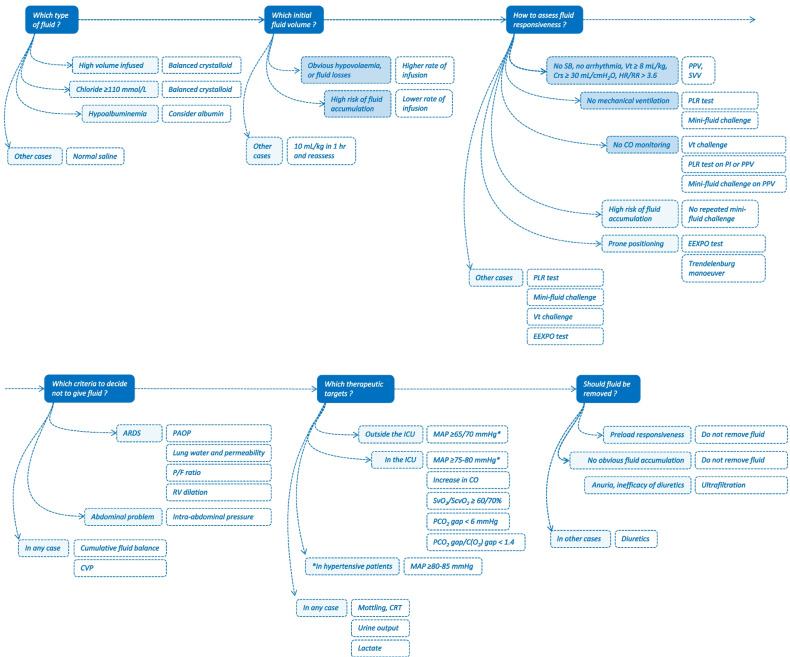
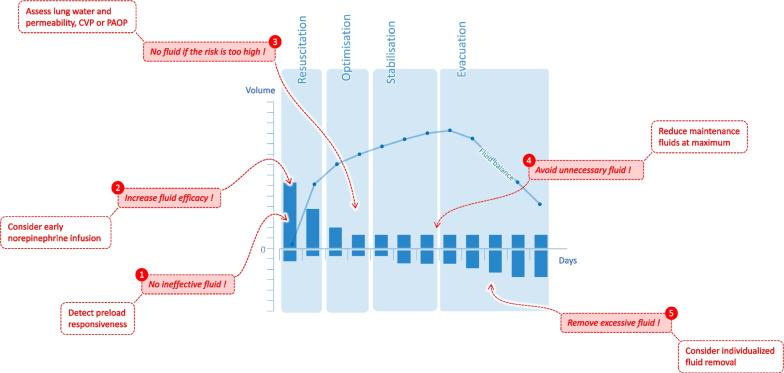
During septic shock, fluid therapy is aimed at increasing cardiac output and improving tissue oxygenation, but it poses two problems: it has inconsistent and transient efficacy, and it has many well-documented deleterious effects. We suggest that there is a place for its personalization according to the patient characteristics and the clinical situation, at all stages of circulatory failure. Regarding the choice of fluid for volume expansion, isotonic saline induces hyperchloremic acidosis, but only for very large volumes administered. We suggest that balanced solutions should be reserved for patients who have already received large volumes and in whom the chloremia is rising. The initial volume expansion, intended to compensate for the constant hypovolaemia in the initial phase of septic shock, cannot be adapted to the patient's weight only, as suggested by the Surviving Sepsis Campaign, but should also consider potential absolute hypovolemia induced by fluid losses. After the initial fluid infusion, preload responsiveness may rapidly disappear, and it should be assessed. The choice between tests used for this purpose depends on the presence or absence of mechanical ventilation, the monitoring in place and the risk of fluid accumulation. In non-intubated patients, the passive leg raising test and the mini-fluid challenge are suitable. In patients without cardiac output monitoring, tests like the tidal volume challenge, the passive leg raising test and the mini-fluid challenge can be used as they can be performed by measuring changes in pulse pressure variation, assessed through an arterial line. The mini-fluid challenge should not be repeated in patients who already received large volumes of fluids. The variables to assess fluid accumulation depend on the clinical condition. In acute respiratory distress syndrome, pulmonary arterial occlusion pressure, extravascular lung water and pulmonary vascular permeability index assess the risk of worsening alveolar oedema better than arterial oxygenation. In case of abdominal problems, the intra-abdominal pressure should be taken into account. Finally, fluid depletion in the de-escalation phase is considered in patients with significant fluid accumulation. Fluid removal can be guided by preload responsiveness testing, since haemodynamic deterioration is likely to occur in patients with a preload dependent state.
Keywords: Cardiac output; Fluid balance; Fluid challenge; Passive leg raising; Tidal volume; Volume expansion.
© 2023. The Author(s).
Conflict of interest statement
XM is a member of the Medical Advisory Board of Pulsion Medical Systems, Getinge, he received fees for scientific lectures from Pulsion Medical Systems, Getinge and Baxter, and limited research grants from Pulsion Medical Systems, Getinge. CL received fees for lectures from Sedana Medical. J-LT is a member of the Medical Advisory Board of Pulsion Medical Systems, Getinge, he received fees for scientific lectures from Pulsion Medical Systems, Getinge, and limited research grants from Pulsion Medical Systems, Getinge.
Figures
Comment in
-
Fluid removal tolerance during the de-escalation phase: is preload unresponsiveness the best guiding candidate?Crit Care. 2023 Apr 20;27(1):154. doi: 10.1186/s13054-023-04444-3. Crit Care. 2023. PMID: 37081541 Free PMC article. No abstract available.
References
-
- Malbrain M, Van Regenmortel N, Saugel B, De Tavernier B, Van Gaal PJ, Joannes-Boyau O, Teboul JL, Rice TW, Mythen M, Monnet X. Principles of fluid management and stewardship in septic shock: it is time to consider the four D's and the four phases of fluid therapy. Ann Intensive Care. 2018;8(1):66. doi: 10.1186/s13613-018-0402-x. - DOI - PMC - PubMed
-
- Evans L, Rhodes A, Alhazzani W, Antonelli M, Coopersmith CM, French C, Machado FR, McIntyre L, Ostermann M, Prescott HC, et al. Executive summary: surviving sepsis campaign: international guidelines for the management of sepsis and septic shock 2021. Crit Care Med. 2021;49(11):1974–1982. doi: 10.1097/CCM.0000000000005357. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
