

An unusual case of a giant fetal facial tumour and review of the literature
- PMID: 36964892
- PMCID: PMC10691997
- DOI: 10.1007/s11845-023-03344-3
An unusual case of a giant fetal facial tumour and review of the literature
Abstract
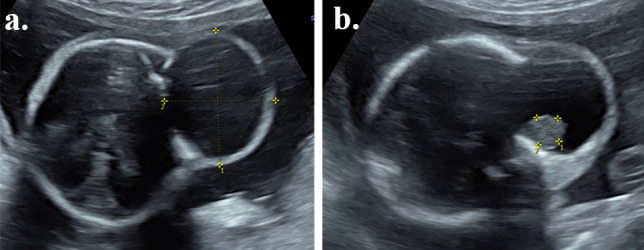
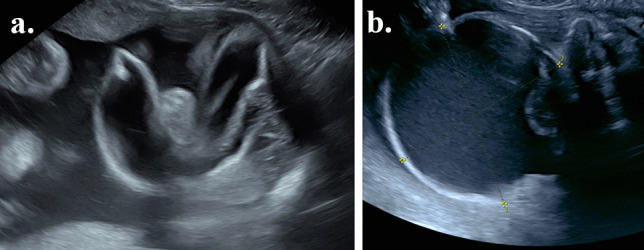
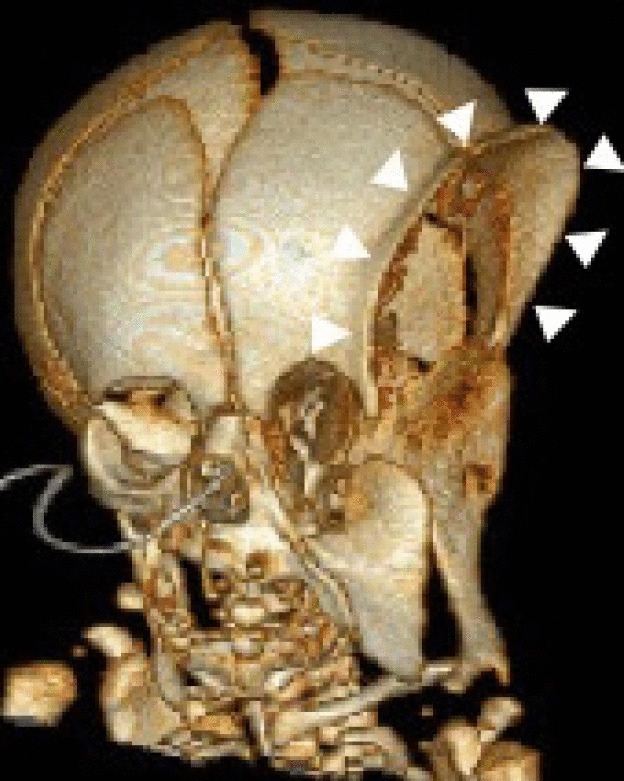
We present the case of a pregnant 32-year-old woman who presented with a giant fetal facial tumour at 22 weeks. The mass, initially 4 × 3.5 × 3 cm in size, was largely cystic with a small solid component. It subsequently increased to 9 × 9 × 10 cm. Significant compression effects on the fetal orbit, temple and infratemporal fossa, with potential compression of the optic nerve, were noted on ultrasound and MRI. The cyst required drainage twice in the pregnancy: firstly to reduce the compression effects and secondly to facilitate caesarean delivery. Postnatally, the baby had significant compression and displacement of the craniofacial skeleton from the mass effect. Postnatal histology revealed a diagnosis of a teratoma. This case highlights the complexities and challenges surrounding the diagnosis and management of a giant fetal facial tumour.
Keywords: Congenital tumour; Fetal anomaly; Fetus; Pregnancy.
© 2023. The Author(s).
Figures





References
-
- Feygin T, Khalek N, Moldenhauer JS (2020) Fetal brain, head, and neck tumors: Prenatal imaging and management. Prenat Diagn 40(10):1203–1219 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
