

Natural History and Predictive Factors of Outcome in Medullary Thyroid Microcarcinoma
- PMID: 36964913
- PMCID: PMC10505538
- DOI: 10.1210/clinem/dgad173
Natural History and Predictive Factors of Outcome in Medullary Thyroid Microcarcinoma
Abstract
Context: Management of sporadic medullary thyroid microcarcinoma smaller than 1 cm (micro-MTC) is controversial because of conflicting reports of prognosis. As these cancers are often diagnosed incidentally, they pose a management challenge when deciding on further treatment and follow-up.
Objective: We report the outcomes of surgically managed sporadic micro-MTC in a specialist endocrine surgery and endocrinology unit and identify associations for recurrence and disease-specific survival in this population.
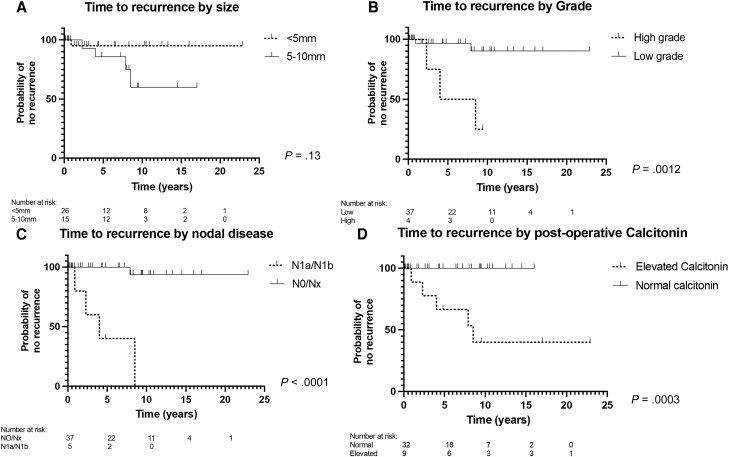
Methods: Micro-MTCs were identified from a prospectively maintained surgery database, and slides were reviewed to determine pathological grade. The primary end points were recurrence, time to recurrence and disease-specific survival. Prognostic factors assessed included size, grade, lymph node metastasis (LNM), and postoperative calcitonin.
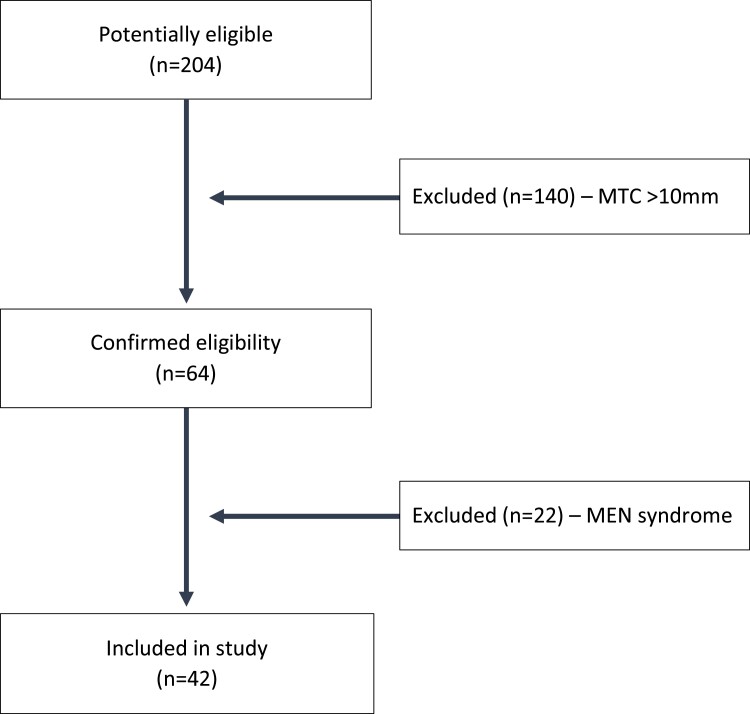
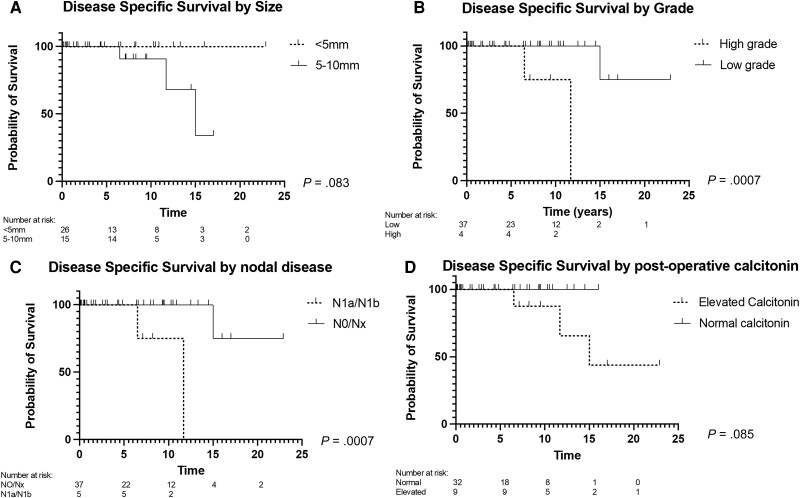
Results: From 1995 to 2022, 64 patients were diagnosed with micro-MTC with 22 excluded because of hereditary disease. The included patients had a median age of 60 years, tumor size of 4 mm, and 28 (67%) were female. The diagnosis was incidental in 36 (86%) with 4 (10%) being high grade, 5 (12%) having LNM and 9 (21%) having elevated postoperative calcitonin. Over a 6.6-year median follow-up, 5 (12%) developed recurrence and 3 (7%) died of MTC. High grade and LNM were associated with 10-year survival estimates of 75% vs 100% for low grade and no LNM (hazard ratio = 831; P < .01). High grade, LNM, and increased calcitonin were associated with recurrence (P < .01). Tumor size and type of surgery were not statistically significantly associated with recurrence or survival. No patients with low grade micro-MTC and normal postoperative calcitonin developed recurrence.
Conclusion: Most sporadic micro-MTCs are detected incidentally and are generally associated with good outcomes. Size is not significantly associated with outcomes. Using grade, LNM, and postoperative calcitonin allows for the identification of patients at risk of recurrence to personalize management.
Keywords: medullary thyroid cancer; medullary thyroid microcarcinoma; outcomes; surgery; tumor grade.
© The Author(s) 2023. Published by Oxford University Press on behalf of the Endocrine Society.
Figures

Comment in
-
Letter to the Editor From Devgan and Mayilvaganan: "Natural History and Predictive Factors of Outcome in Medullary Thyroid Microcarcinoma".J Clin Endocrinol Metab. 2023 Dec 21;109(1):e433. doi: 10.1210/clinem/dgad379. J Clin Endocrinol Metab. 2023. PMID: 37378844 No abstract available.
References
-
- Pillarisetty VG, Katz SC, Ghossein RA, Tuttle RM, Shaha AR. Micromedullary thyroid cancer: how micro is truly micro? Ann Surg Oncol. 2009;16(10):2875‐2881. - PubMed
-
- Valle LA, Kloos RT. The prevalence of occult medullary thyroid carcinoma at autopsy. J Clin Endocrinol Metab. 2011;96(1):E109‐E113. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
