

Longitudinal Lung Function Assessment of Patients Hospitalized With COVID-19 Using 1H and 129Xe Lung MRI
- PMID: 36965765
- PMCID: PMC10036146
- DOI: 10.1016/j.chest.2023.03.024
Longitudinal Lung Function Assessment of Patients Hospitalized With COVID-19 Using 1H and 129Xe Lung MRI
Abstract
Background: Microvascular abnormalities and impaired gas transfer have been observed in patients with COVID-19. The progression of pulmonary changes in these patients remains unclear.
Research question: Do patients hospitalized with COVID-19 without evidence of architectural distortion on structural imaging exhibit longitudinal improvements in lung function measured by using 1H and 129Xe MRI between 6 and 52 weeks following hospitalization?
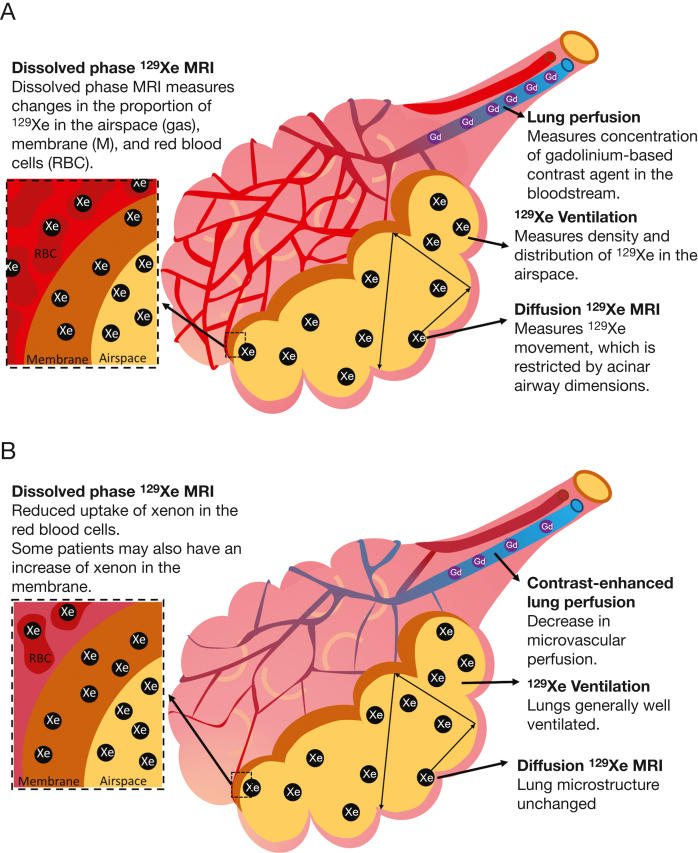
Study design and methods: Patients who were hospitalized with COVID-19 pneumonia underwent a pulmonary 1H and 129Xe MRI protocol at 6, 12, 25, and 51 weeks following hospital admission in a prospective cohort study between November 2020 and February 2022. The imaging protocol was as follows: 1H ultra-short echo time, contrast-enhanced lung perfusion, 129Xe ventilation, 129Xe diffusion-weighted, and 129Xe spectroscopic imaging of gas exchange.
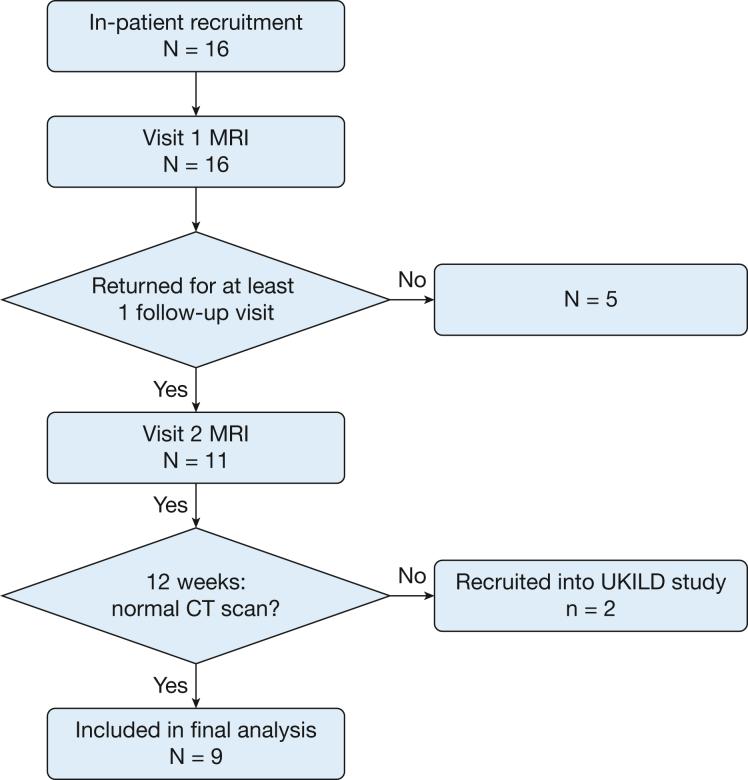
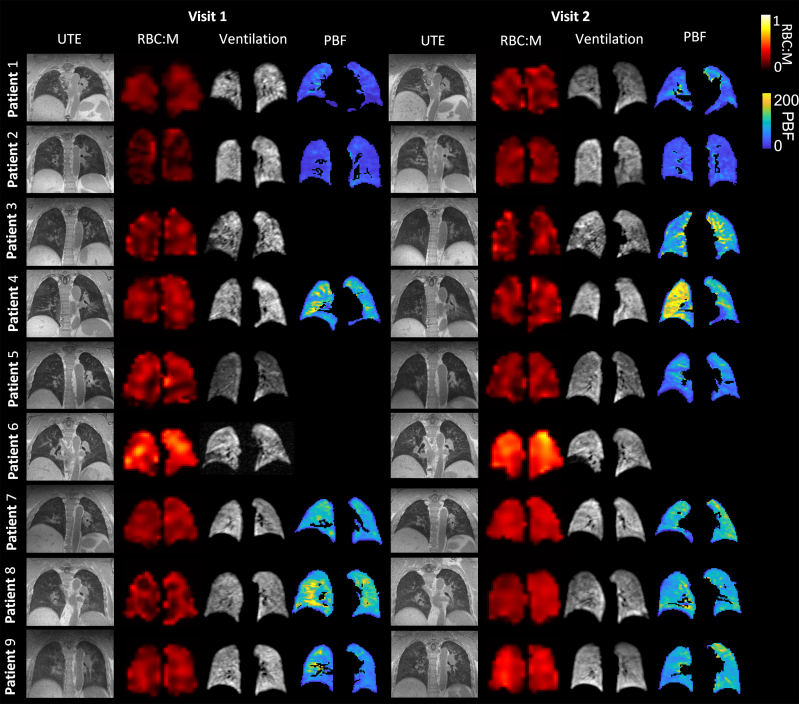
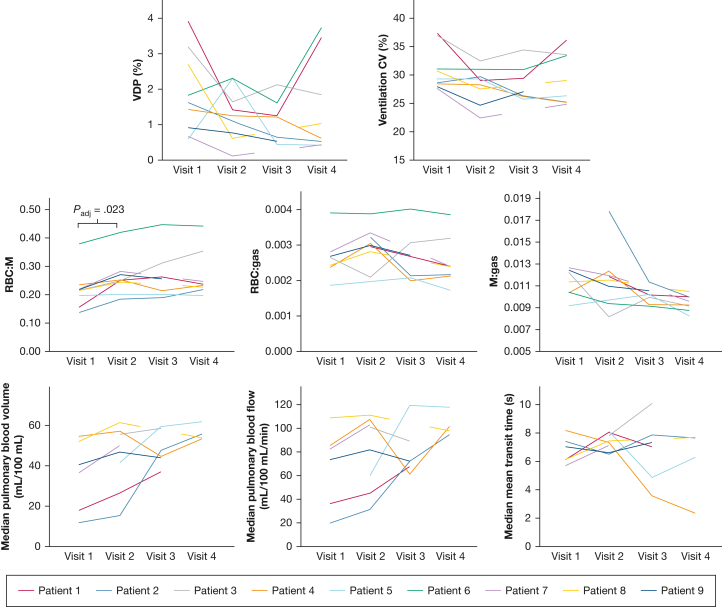
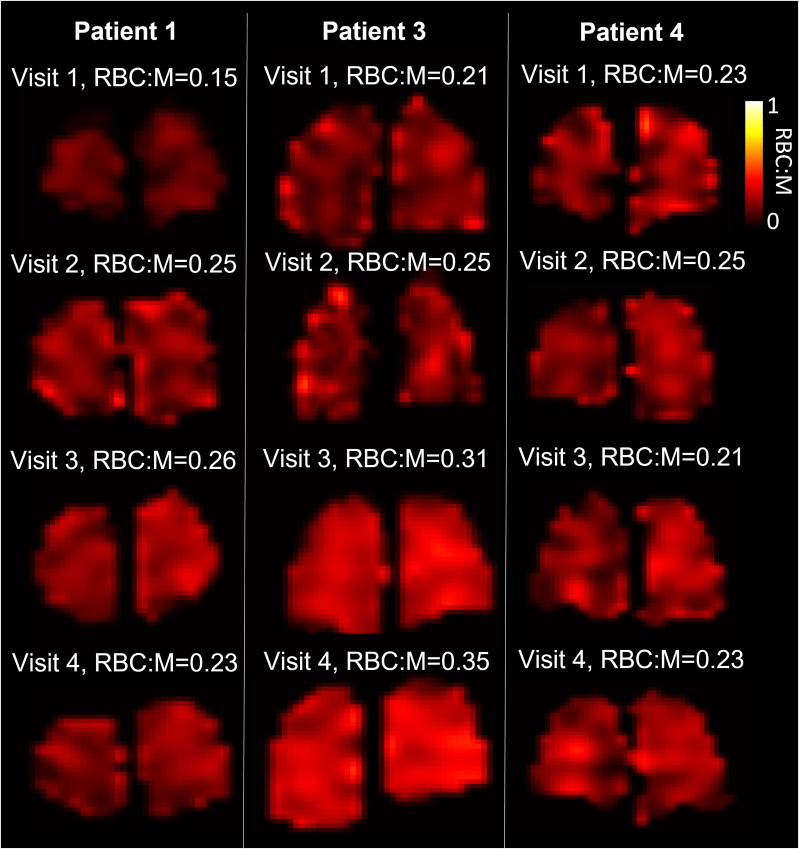
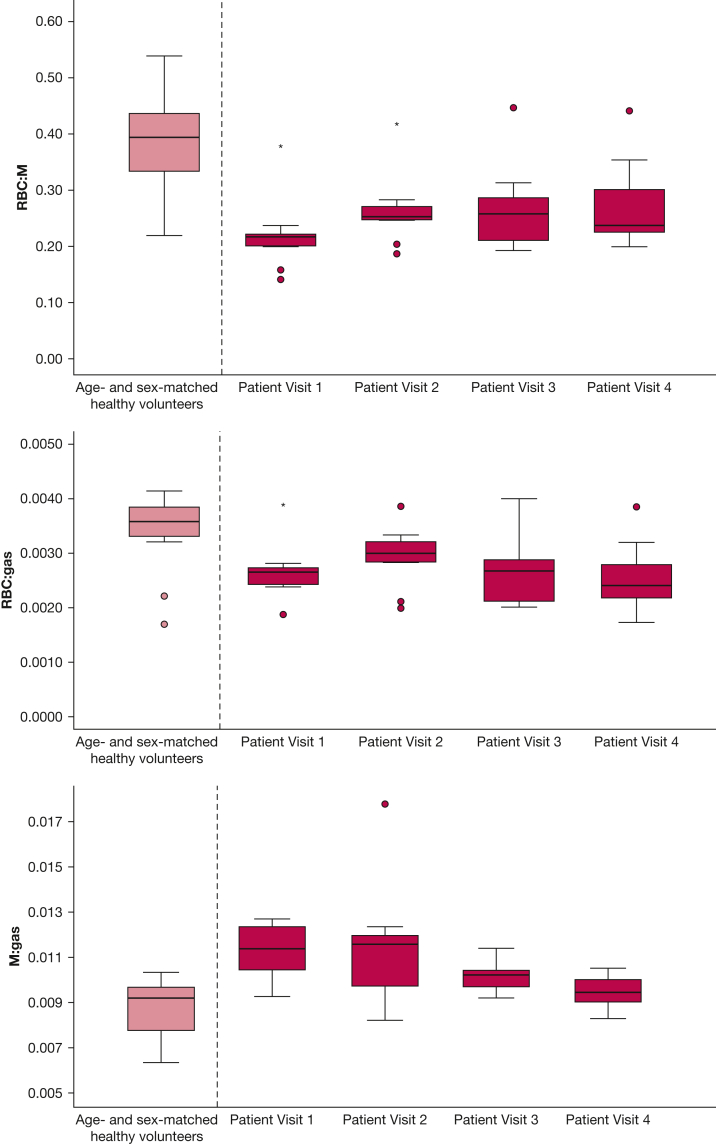
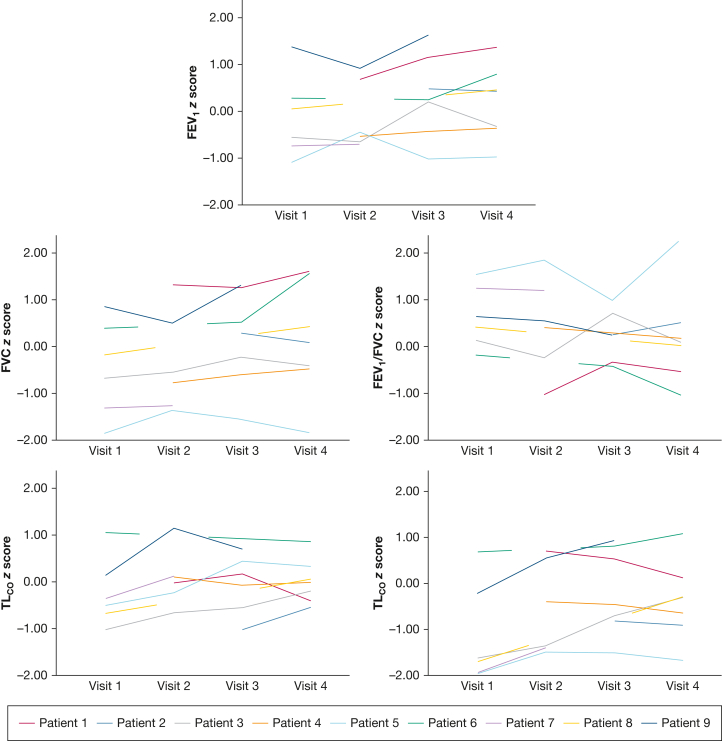
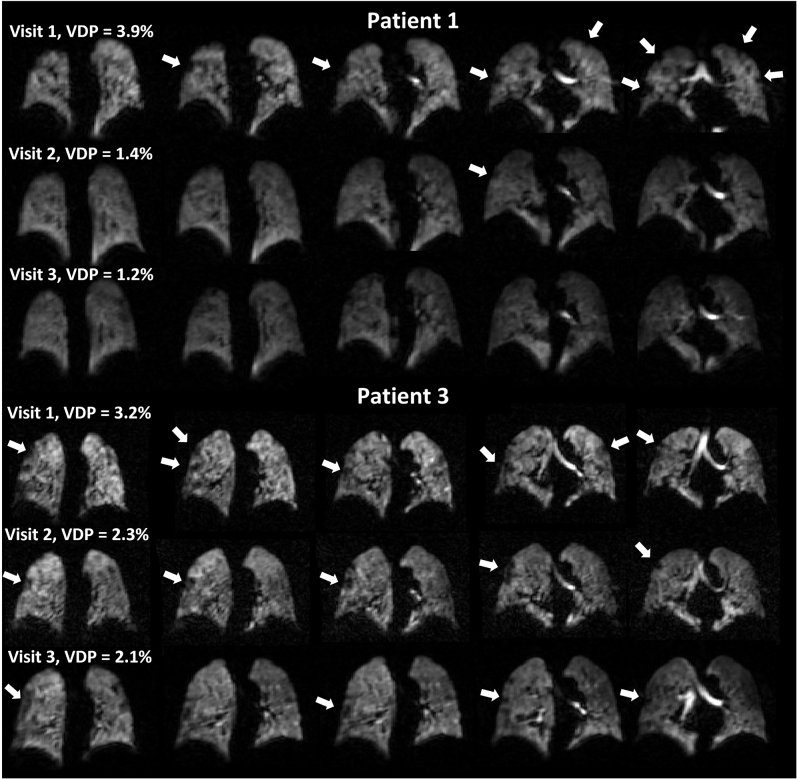
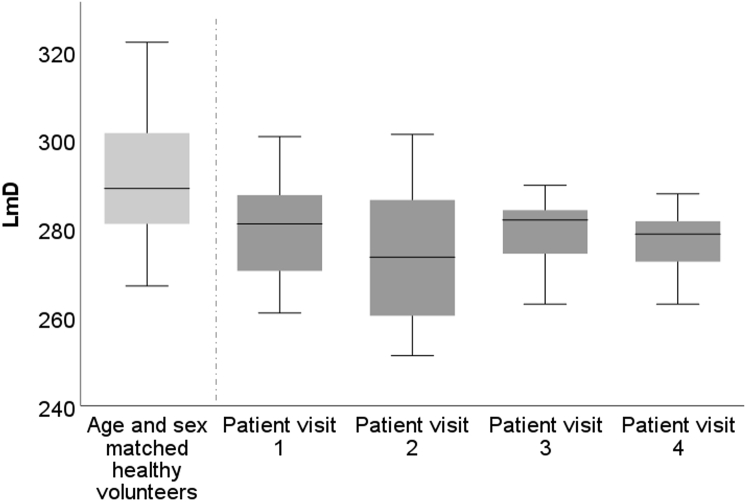
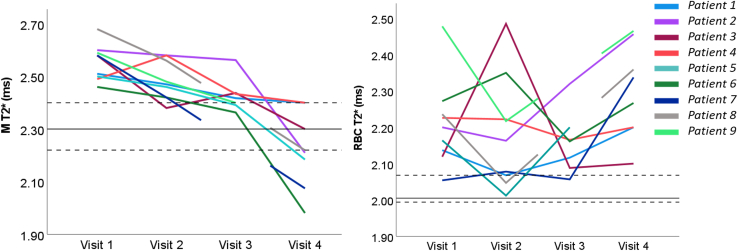
Results: Nine patients were recruited (age 57 ± 14 [median ± interquartile range] years; six of nine patients were male). Patients underwent MRI at 6 (n = 9), 12 (n = 9), 25 (n = 6), and 51 (n = 8) weeks following hospital admission. Patients with signs of interstitial lung damage were excluded. At 6 weeks, patients exhibited impaired 129Xe gas transfer (RBC to membrane fraction), but lung microstructure was not increased (apparent diffusion coefficient and mean acinar airway dimensions). Minor ventilation abnormalities present in four patients were largely resolved in the 6- to 25-week period. At 12 weeks, all patients with lung perfusion data (n = 6) showed an increase in both pulmonary blood volume and flow compared with 6 weeks, although this was not statistically significant. At 12 weeks, significant improvements in 129Xe gas transfer were observed compared with 6-week examinations; however, 129Xe gas transfer remained abnormally low at weeks 12, 25, and 51.
Interpretation: 129Xe gas transfer was impaired up to 1 year following hospitalization in patients who were hospitalized with COVID-19 pneumonia, without evidence of architectural distortion on structural imaging, whereas lung ventilation was normal at 52 weeks.
Keywords: (129)Xe; COVID-19; MRI; gas transfer; hyperpolarized gas; imaging; xenon MRI.
Copyright © 2023 The Author(s). Published by Elsevier Inc. All rights reserved.
Figures
Comment in
-
The Proton Is Not Enough: Opportunities of Combined Multinuclear MRI for Lung Functional Imaging.Chest. 2023 Sep;164(3):572-573. doi: 10.1016/j.chest.2023.03.038. Chest. 2023. PMID: 37689468 No abstract available.
References
-
- Loo J., Spittle D.A., Newnham M. COVID-19, immunothrombosis and venous thromboembolism: biological mechanisms. Thorax. 2021;76(4):412–420. - PubMed
-
- Attaway A.H., Scheraga R.G., Bhimraj A., Biehl M., Hatipoglu U. Severe Covid-19 pneumonia: pathogenesis and clinical management. BMJ. 2021;372:n436. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
