

Cost-effectiveness of early rhythm control vs. usual care in atrial fibrillation care: an analysis based on data from the EAST-AFNET 4 trial
- PMID: 36966734
- PMCID: PMC10227663
- DOI: 10.1093/europace/euad051
Cost-effectiveness of early rhythm control vs. usual care in atrial fibrillation care: an analysis based on data from the EAST-AFNET 4 trial
Abstract
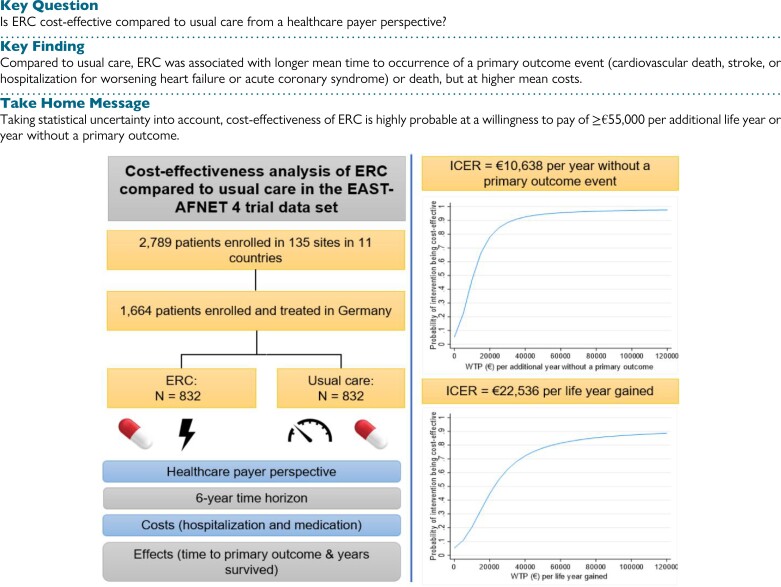
Aims: The randomized, controlled EAST-AFNET 4 trial showed that early rhythm control (ERC) reduces the rate of a composite primary outcome (cardiovascular death, stroke, or hospitalization for worsening heart failure or acute coronary syndrome) by ∼20%. The current study examined the cost-effectiveness of ERC compared to usual care.
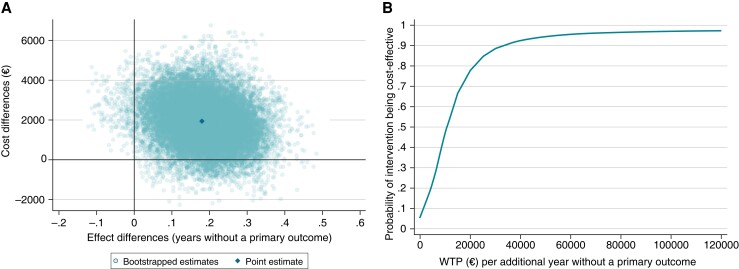
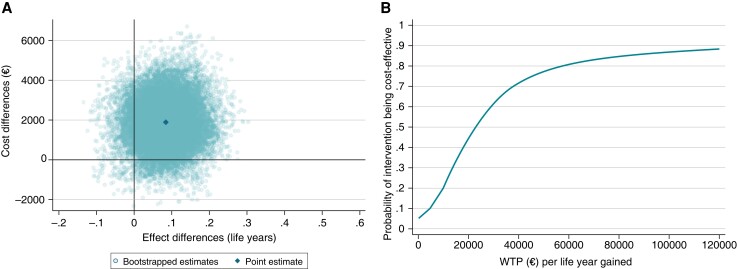
Methods and results: This within-trial cost-effectiveness analysis was based on data from the German subsample of the EAST-AFNET 4 trial (n = 1664/2789 patients). Over a 6-year time horizon and from a healthcare payer's perspective, ERC was compared to usual care regarding costs (hospitalization and medication) and effects (time to primary outcome; years survived). Incremental cost-effectiveness ratios (ICERs) were calculated. Cost-effectiveness acceptability curves were constructed to visualize uncertainty. Early rhythm control was associated with higher costs [+€1924, 95% CI (-€399, €4246)], resulting in ICERs of €10 638 per additional year without a primary outcome and €22 536 per life year gained. The probability of ERC being cost-effective compared to usual care was ≥95% or ≥80% at a willingness-to-pay value of ≥€55 000 per additional year without a primary outcome or life year gained, respectively.
Conclusion: From a German healthcare payer's perspective, health benefits of ERC may come at reasonable costs as indicated by the ICER point estimates. Taking statistical uncertainty into account, cost-effectiveness of ERC is highly probable at a willingness-to-pay value of ≥€55 000 per additional life year or year without a primary outcome. Future studies examining the cost-effectiveness of ERC in other countries, subgroups with higher benefit from rhythm control therapy, or cost-effectiveness of different modes of ERC are warranted.
Keywords: Atrial fibrillation; Cost-effectiveness; Early rhythm control.
© The Author(s) 2023. Published by Oxford University Press on behalf of the European Society of Cardiology.
Conflict of interest statement
Conflict of interest: H.JGM.C. reports support to institution from Medtronic, Cardialysis, Acesion Pharma, and InCarda Therapeutics and fees from Roche Diagnostics, Daiichi-Sankyo, and Sanofi, all outside the submitted work. P.V. receives consultant fees from Hygeia Hospitals Group, HHG, Servier International, and European Society of Cardiology. AJ.C. reports personal fees from Bayer, Daiichi Sankyo, Menarini, Pfizer, Sanofi, Medtronic, Abbott, and Boston Scientific. K.W. reports support to institution from the German Federal Ministry for Education and Research (BMBF), Atrial Fibrillation NETwork (AFNET), German Centre for Cardiovascular Researcher, EU Horizon 2020, and Biotronik and personal fees from Biotronik, Boston Scientific, and Novartis, all outside the submitted work. A.R. received consultant fees from Medtronic, KODEX-EPD, and Biosense Webster and travel grants and lecture fees from Medtronic, Cardiofocus, Biosense Webster, Abbott, Boehringer Ingelheim, Philips KODEX-EPD, Ablamap, Bayer, and Novartis. P.K. receives research support for basic, translational, and clinical research projects from the European Union, British Heart Foundation, Leducq Foundation, Medical Research Council (UK), and German Centre for Cardiovascular Research and from several drug and device companies active in atrial fibrillation and has received honoraria from several such companies in the past, but not in the last 3 years. He is listed as inventor on two patents held by the University of Birmingham (Atrial Fibrillation Therapy WO 2015140571, Markers for Atrial Fibrillation WO 2016012783). All remaining authors have declared no conflicts of interest.
Figures
Comment in
-
Early rhythm control for atrial fibrillation: looking cost-effective, at least from one direction.Europace. 2023 May 19;25(5):euad085. doi: 10.1093/europace/euad085. Europace. 2023. PMID: 36994788 Free PMC article. No abstract available.
References
-
- Magnussen C, Niiranen TJ, Ojeda FM, Gianfagna F, Blankenberg S, Njolstad Iet al. . Sex differences and similarities in atrial fibrillation epidemiology, risk factors, and mortality in community cohorts: results from the BiomarCaRE consortium (biomarker for cardiovascular risk assessment in Europe). Circulation 2017;136:1588–97. - PMC - PubMed
-
- Wolf PA, Abbott RD, Kannel WB. Atrial fibrillation as an independent risk factor for stroke: the Framingham Study. Stroke 1991;22:983–8. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
